I’m glad to see this and we need to concentrate on speeding this process up. This isn’t the last pandemic and all things considered this one was a pretty benign one to have to fight. The next one might not just kill mainly the old and weak and might need much more than a mask (that we still can’t get people to wear!) to prevent its spread. Hopefully before then, we can work to get everyone more on the same page and have a rapid vaccine task force ready.
My brother is a doctor and he got his Pfizer shot yesterday. Less than one year has passed since the first case in the USA. I consider this one of the great accomplishments of science. It will go unnoticed by many idiots on social media but it is an amazing achievement by all the scientists and doctors involved.
To get worse than COVID you'd need a virus that takes a long time to develop symptoms and then has a high death rate. In that scenario there would be a lot more public fear and we'd have an easier time keeping people at home. So I'm still of the opinion it's harder to have a worse situation than COVID.
Yeah this pandemic has been described as the perfect middle ground for politicization, denialism, and just laissez-faire attitudes.
Any more deadly (like Ebola) it becomes incredibly scary and people likely do whatever it takes when they see people around them dropping like flies (especially in horrific ways).
Any less deadly (basically the yearly flu) and it becomes easy to ignore and just becomes part of the background process.
COVID is somewhere in between. Deadly enough that hundreds of thousands of people are dying unnecessarily. But can still feel a million miles away for so many people.
Was it not though? I assume you'd want a pandemic deadly enough for that convinces a majority of the populace that it's a serious event (to encourage downstream change to better prepare for a worse pandemic), while at the same time not causing people to drop like flies. As you stated, anything less severe would be taken less seriously. To have something to be taken more serious, it has to be more deadly.
Despite the denialism we currently have, it seems to have made the world recognize the importance of preparation.
"more deadly" does not necessarily mean more deaths in this case. If it kills like ebola more folks could take it seriously ultimately resulting in lower transmission and death rates.
In particular, when COVID19 was first spreading but we knew about it back in February countries could've easily contact traced to flush it out and then quarantined all incoming travelers to keep it out.
But most countries deemed those actions too extreme and economically damaging so instead let it come spread and do way more damage.
Also taking into account that often the balance between spreading the disease and letting people work to feed themselves and loved ones is a massive challenge.
In my country we have destroyed economiy due to 10 years of incompetent greedy politics which had killed it already. People are out of work because of that.
Now the pandemic has made sure no one will recover at an acceptable rate, because new politicians also struggle to find the balance.
At this side of the planet we are screwed at such a hard rate, its amazing I can still feed myself, pay utilities and internet and be medically insured
What you're proposing is highly experimental and probably wouldn't work. There's no single country in the world that has been able to restrain the sars2 virus despite spending millions trying to do so.
Seriously, we can't expect to match the performance of a low income country we bombed back to the stone age just a few decades ago?
Vietnam isn't a paragon of wealth and competent administration today, there is no good reason our public health departments should not have been able to perform equally or better than their equivalents in Vietnam.
Other than Australia, China, New Zealand, and Vietnam, you mean? And China managed that after it had already spread widely domestically; the others were quick on their feet.
Cambodia too. We had our first known case of community transmission three weeks ago. It topped at 41 cases and we’ve had no new ones for three days.
We have mandatory two week quarantine for all arivals, stores lose their business licenses if they let anyone in without a mask. Schools, cinemas, gyms, clubs are all closed.
We’re hoping things will open up again in two weeks.
Ah yes, "warned", by assuring us that the virus was no worse than the common cold, and we were rapidly "turning a corner", and that it would just "go away on its own".
> wanted to close the borders
If he really wanted to, what stopped him? He was clearly fully capable of closing borders, given that he did close the border to China (too late) and Europe (also too late). Where was the closure to South Korea when the virus was spiking there?
"Ah yes, "warned", by assuring us that the virus was no worse than the common cold, and we were rapidly "turning a corner", and that it would just "go away on its own"."
I suppose he shouldn't have listened to the WHO at the time, which told us it couldn't spread from human-to-human. Nobody really knew anything about the virus at the time, except China, and the lied about it...but orange man bad.
He was also being impeached at the time and the Democrats were too busy with this to care about the potential spread of Covid-19.
He also talked about hydroxychloroquine, which his doctor was using at the time as a preventative measure for Covid-19.
Was it a cure? No (he never said it was), but Doctors were taking it at the time and many were still were taking it before the vaccine.
Because everything Trump said is bad, it was equated with junk science and possibly lead to the deaths of many more people.
"If he really wanted to, what stopped him? He was clearly fully capable of closing borders, given that he did close the border to China (too late) and Europe (also too late). Where was the closure to South Korea when the virus was spiking there?"
Right. He could easily just make decisions without the Democrats using everything in their power to stop him. Where have you been the last 4 years?
Again, The WHO was warned about this back in December from Taiwan officials.
Trump has been stopped from making decisions every step of the way from the Democrats and then Demonized in the press (which spread false information to the masses).
You really can't then blame him for making the wrong decision.
"It’s going to go away, hopefully at the end of the month. And, if not, hopefully it will be soon after that."
— Trump, 2020-03-31
That's long after human-to-human transmission was confirmed. So, no, you can't blame the WHO there.
> Right. He could easily just make decisions without the Democrats using everything in their power to stop him.
...Uh okay? Since when has Trump cared what Democrats thought? Again, why did he not attempt to close the South Korean border if he cared so much? I'll tell you why: it's because Trump was just looking for an excuse to close the border to a country he already didn't like. He never cared about the virus, only about his personal agenda.
The China border was “closed” yet we had tens of thousands of Chinese travelers enter the US straight after the closure.
And the European border “closing” was so badly managed that it almost certainly seeded the massive outbreak in the NorthEast in the initial phase by causing hundreds of super spreader events daily in airports across the northeast as people all tried to return from Europe within the same few days and the airports were completely unprepared to handle them safely.
Most countries were unprepared, except for Taiwan. The government of China lied about SARS outbreaks and Taiwan has since had scientists that study disease outbreaks in China. Covid was spotted in December, but the WHO is under the influence of China and didn't listen.....
It's strange how the Chinese government: lied about the disease, allowed it to spread throughout the world without warning anyone, and purchased all of the PPE (creating a shortage and possibly causing even more deaths).
MERS (which didn't reach the US) was probably a better "training pandemic" because of the high rate of symptoms early on in the infection. One could take drastic measures to isolate the infected and prevent many deaths.
It didn't cause billions of people to gain experience in stocking up on supplies, learning how to live while locked down and the problems it entails, and wearing masks and taking other precautions. Therefore, it didn't serve as a training pandemic, except maybe for a small group. (It seems it did serve as training for vaccine developers, at least.)
It was a good "training pandemic". Some countries did quite well (Taiwan, Japan, Vietnam, New Zealand, etc.) and some countries did poorly (the US, Brazil, parts of Europe). Overall, being able to develop and deploy a vaccine within a calendar year seems like a success. Though a lack of inexpensive, quick, home administered tests seems like kind of a failure - they exist, but they haven't been backed by governments to the point where they can be manufactured in large numbers.
Ebola requires direct contact with bodily fluids, it's not nearly as easily transmittable as Covid. Note that seasonal flu levels are at historic lows [1, 2], despite Covid raging to the point where many US states' ICUs are filled to capacity.
The more deadly a virus is the less likely you will have super spreaders. If the virus was 5x deadly you would probably also see 5x worse symptoms in most people. So instead of taking a bunch of DayQuil and going to the business meeting that person would be home feeling and looking like shit.
> The more pain we suffer now, the longer the lesson will last.
More evidence of the pervasive political attitude that’s “science-based” but more like modern day fundamentalist fire-and-brimstone “anyone smiling wrought all the suffering in the world” Christianity.
If the death rates in children vs. elderly were reversed with COVID, all hell would have broken loose. There is nothing people are more protective over than their kids. Behavior would have been completely different.
I was in SE Asia when H1N1pdm9 hit. There were 60m cases in the US that year, and 14,000 deaths that year in the US, and 75,000 deaths since 2009. It predominantly affected younger people[1], and barely hit elderly people. The CDC estimates it killed 150k to 500k people the first year it circulated across the world. I was wearing a mask in Macau, and my kids aged 12 and 9 years-old in the US at the time were not as almost all Americans were not wearing masks. The WHO declared an end to the pandemic in August 2010, but it causes illness, hospitalizations, and deaths each year as a seasonal flu the same way COVID-19 probably will in the coming years.
I believe there's been a misunderstanding where people think COVID is more dangerous to elderly people because they just tend to be generically vulnerable to a lot of disease.
That's not the case, however. If you compare death rates within different age groups, the risk for elderly is dramatically higher, even in comparison to other diseases that tend to be worse in old age (yes, exactly, such as the flu).
Even though it's less dangerous for young people, there's still reports that it was the top cause of death for people in their 20s or 30s this summer. The absolute numbers aren't that high, but it turns out people in their 20s and 30s don't die randomly that often either.
It also depends on how one defines danger. Would you rather die a few years earlier in your old age? Or live with reduced lung capacity for many years? And how common is that with COVID19?
We're still waiting to see the fall-out of long COVID.
You say this now but if we ask you then, the day of your death, would you rather die now or live a few more years in a diminished capacity, you might have a very different answer.
If you told anyone, on their death bed, "if you had run 25 km a week since [n-15 years] you would have been able to move better / dance with pretty girls / play [tennis | golf | etc] until two years ago," I think most people would say WHY DIDN'T YOU TELL ME.
True. But the data to date indicates that it boils down to marginalized vs not. Covid has done well with nursing homes and lower socioeconomic minority communities. People absolutely care about the children. But they care about what threatens them directly as well.
The profile to date is not close enough to home for most (white) middle class Americans. But that lack of fear to some extent, at this point, is statistically justified. That is, once you get outside the sweet spot the chance of death declines.
The virus is real. The deaths are real. However, despite the media hyperbol (and complete lack of basic lack of understanding of data and data analysis) how those deaths are distributed is uneven. Very much so.
Honestly, kids are just fine with it. Anecdotally, they are managing far better than adults. Not oblivious to the situation, but far more adaptable to just staying at home.
History rhymes and we are doing our best.
Please don't blame others ala "Those who ignore the past are doomed to repeat the mistakes"...
We will have much more possibilities and views in the future though and are currently blind(er) compared to that.
Or COVID! There's been some reports about long term damage to people's lungs and such. To be frank, that's what scares me a lot more than the acute disease as someone who's still relatively young.
It seems to be at least a few percent of all cases. A majority of cases which are hospitalized have long-term effects too. It's also common enough that anecdotally -- I'm in a city hit hard and early by COVID. I can't tell you if it's 30% or 2%, but it's definitely not 1:10,000.
There’s no evidence to suggest COVID causes serious damage to those with minor to medium level symptoms. When the media talks about lung damage they seem to be talking about those who nearly died from the disease.
Not trying to minimise the seriousness of COVID, but simply suggesting there is no evidence of serious long term impact to the majority of cases.
I know of three colleagues who had minor cold like symptoms, 2/3 still talk about being winded climbing stairs, and both are physically fit 30 somethings.
I think lack of evidence is more a symptom of limited information.
Not lost on me that despite being a rare disease I know five people that have had guillain barre syndrome[1]. And I know about ten people who appear to have some sort of chronic malaise. I suspicious those are the result of viral infections.
There is also the minority opinion that some forms of dementia are due latent viral infections.
[1] You don't guillain barre syndrome takes years to recover and is absolutely traumatic.
Kind of related - most people probably don’t know, but the first studies around “zombie apocalypse” were just that, simulations of a bad virus outbreak.
Better yet, a virus (or some other kind of infectious agent, how about a fungus next?) that spreads rapidly but has no symptoms, and may lay dormant for over a year until it receives certain infrequent but not rare triggers, upon which it kills the host quickly.
Let's say pregnancy, a new Star Wars movie, or birth; transferred from parent to child, "activates" inside the newborn and then kills the parents too.
> They identified the sequence for the spike protein, plugged that into their vaccine platform, and voila – an mRNA vaccine against the SARS-CoV-2 virus.
Moderna zeroed in on the spike protein thanks th large amount of previous research on SARS-CoV-1. Vaccines effective in animal models of SARS were developed based on this approach starting around 2004:
> The win-win here, however, is that the more we develop a universal vaccine platform, the more we can have the best of both worlds – fast plus safe and effective. But this also means we need public buy in, which requires reassuring the public about the process and the strategy. It also means reassuring the public that the process has not been politicized, and that objective experts are driving (something the TA did poorly).
The MRNA approach requires an understanding of viral vulnerabilities and a lot of animal studies prior to the synthesis of a vaccine candidate. Again, that seemingly fruitless work with SARS more than a decade ago was the key to the success of Moderna and Pfizer today.
It's a lesson that should not be forgotten but probably will.
The other thing to keep in mind is that the Pfizer and Moderna approvals represent the first ever large-scale use of MRNA vaccines in humans. That substantially lowers the barrier to entry of new vaccines based on the same platform.
The idea that while it may have taken only a few days, it still wasn't "easy" is probably best demonstrated by the Pfizer/BioNTech joint venture: Pfizer has tens of thousands of biologist of any stripe working for them, but they chose to partner with a comparatively tiny startup that had the expertise to design the vaccine.
Actually the partnership came together the other way round: the "comparatively tiny startup" saw articles about SARS-CoV-2, decided to start sketching out a vaccine, called Pfizer, which they had prior business relations due to joint work on previous projects, asked whether they'd be interested in jointly develop this new vaccine, and Pfizer's head of vaccine research said "yeah, sure!" immediately.
That would require the kind of understanding of viral vulnerabilities I'm thinking of. The same applies to any virus, of course.
To my knowledge, that kind of understand does not exist because coronaviruses have been largely ignored historically, with the exception of SARS and MERS.
And we've been trying for decades to get a broad-spectrum or even single-dose-forever vaccine for the flu, so far without much to show for it.
The layman's explanation I've seen about how these mRNA vaccines work is that they get some of your cells to manufacture a protein that is characteristic of the virus, which the cells release and the immune system takes care of.
Then later if you get the virus, the immune system already recognizes that protein and takes care of the virus.
Question: why do we need to have our cells make the protein? Couldn't we synthesize and distribute the protein itself and inject that?
Question 2: what happens to the cells that take in the mRNA and make the protein? Do they just make a certain amount of it, then go back to normal?
Or do they keep making it for the lifetime of the cell, and stop doing whatever that cell is normally supposed to do?
Or do they get killed doing this, much like if they were infected by the virus (except, of course, that unlike the with the virus, what they are making is not viral, so the maximum number of cells that would be killed making the protein is equal to the number of mRNA strands in the injection)?
Proteins are chemical compositions - useful machines. Each one (especially outside the context of a cell) requires custom environments to be kept stable. And the processes to manufacture them require other organisms - from which you must now purify that (unstable) protein. And it’s not self-replicating so if you need weekly doses of Ng of material for X doses, you need to produce that much material. RNA solves all of these issues. RNA is a template of common composition that can encode any protein (same chemistry, but in different orders can encode for any arbitrary protein). It can be synthesized in a chemically defined system. And it can persist long enough to produce many generations of proteins. And it can even sometimes be designed to be self replicating. From a theoretical perspective it’s so much better than delivering a custom-purified shot to your blooodstream - different for each virus.
The second question is the hard part - delivery. With the advent of ‘gene therapies’ we needed easy to deliver DNA and RNA to living human cells. We’ve come a long way here and have a number of technologies (oftentimes co-opted from viruses) that range from permanent integration into the cell’s genome (lentivirus) to transient (AAV [see Oxford’s vaccine]) to chemical transfection (Pfizer and Moderna). The RNA in these vaccines is chemically more stable than normal RNA, so it will have half-lives of weeks rather than hours inside cells - but it will degrade after a time and the cells will no longer produce the protein. Proteins in a cell have half-lives of hours to days and even stabilized RNA will be less than a month. After that the material produced by this 'vaccine' will be degraded and gone. However, at that point, the immune system will have permenantly 'encoded' antibodies for the shape of the produced spike protein.
What changes are made to mRNA in these vaccines to make them last longer? Also wouldn't our immune system attack it as foreign then? It seems to me as a layperson that this must have been a key novel and clever part to make these vaccines work. I'd like to read more but don't know where to start.
It's not just proteins. The cells infected with the mRNA present those proteins on the outside of the cell to be recognized by other cells which start a chain process.
He goes through the entire biochem process. Even the cells infected with the mRNA will need to be removed by the immune system using cytotoxic T-cells, so they need to get the chain process going.
The reason we have "memory" for viruses is because a ton of random stuff in our immune systems evolved to multiply exponentially when they come in contact with viruses or proteins that indicate certain infections. It's a lot of stuff and you can't just inject that memory in; you have to stimulate the immune system to create them at a very large scale.
It's not just antibodies. There are memory T-cells, parts of the complement system that get activated; a whole host of things.
My issue is that our immune systems are incredibly complex, and there are a lot of components to this "memory" that are not entirely understood. Every other vaccine is an inactivaed virus (via heat treatment) or attenuated (virus run through other hosts to make it less dangerous to humans). The first vaccine was just a close relative: cow/horse pox instead of smallpox. The former are not dangerous in humans, but seem to produce the same immune memory.
The mRNA vaccines are at attempt to say, "Let's strip out all that other stuff and find just the thing we need." But our immune systems are incredibly complicated. It will be interesting to see if these things actually work at scale.
The trials were to make sure the vaccine is safe in a short about of time. It's not really going to test effectiveness until deployed at scale.
That's not very true. Phase II trials are designed test safety, phasE III trials are designed to test efficacy.
Statistics is advanced (and magic) enough that we're now reasonably sure that the vaccine has a 95% efficacy. That's not 'totally sure', we'll only be totally sure it works once everyone is vaccinated and the pandemic stops. But we _know_ it works, in the scientific-probabilistic meaning of knowledge.
1. One advantage of the mRNA vaccine is that each strand of mRNA is translated to protein many times before it is degraded. So less vaccine has to be manufactured and the dosage can be smaller. Another advantage is that since it lacks proteins you do not develop immunity to the vaccine itself, meaning that you can receive multiple booster doses.
2. Yes, the mRNA is ultimately degraded. But part of the process of developing the vaccine is fine tuning the precise rna sequence in order to achieve the desired half life.
The technology was years in the making. DARPA was also involved.
“In October 2013, DARPA awarded Moderna up to approximately $25 million to research and develop potential mRNA medicines as a part of DARPA’s Autonomous Diagnostics to Enable Prevention and Therapeutics, or ADEPT, program”
But it is very interesting that mRNA vaccines can be very quickly developed for new viruses. The underlying technology may have taken years, but it can be applied to new viruses as soon as the virus is sequenced.
I think this is the silver lining for this pandemic. Covid-19 is lethal, I'm not discounting that, but in terms of real lethality, this was a good test run to show that this approach works. (At least in my lay person's knowledge.) What really scares me are the highly lethal flu strains (I think H5N5?) The fact that we can produce a vaccine this quickly now gives me hope when we encounter a scenario like out of the movie Contagion.
High lethality is often associated with reduced transmissibility. Which makes sense - dead people certainly aren't going to cough on you.
In a Sci Fi movie maybe the virus has a long delay, you're infectious for a month with no symptoms, then drop dead in seconds. But in the real world that's less likely the more extreme it gets.
One thing that did make this virus more dangerous was that many humans became infectious significantly before they realised they had symptoms. With some viruses you get symptoms, then (sometimes as a result of the symptoms) you become infectious, making it easier for public health messages to be effective. "Stay at home if you have symptoms" is extremely effective if people aren't vectors until 12-24 hours after the symptoms are obvious, but almost useless if they're infectious a week earlier.
I'd argue that countries which think the lesson is "We developed a vaccine quickly, good job" are mistaken. The lesson was just, "Elimination strategy works" and the many countries that didn't even attempt that got lucky they weren't decimated for their incompetence.
In many ways, this was a worst case scenario for countries without a history of fighting respiratory diseases. It’s lethal enough to rack up a significant body count, but “safe” enough for large portions of the population to disregard the risk and potentially transmit it. Oh, and it’s airborne and you’re infectious before you have symptoms.
Ironically, a disease with a much higher case fatality rate probably would’ve killed fewer Americans, since we’d be more aligned on stopping it, and it would have a greater tendency to burn itself out.
> Ironically, a disease with a much higher case fatality rate probably would’ve killed fewer Americans, since we’d be more aligned on stopping it
Not unless it was much higher, like 10% whole population fatality might do it but merely twice as much death wouldn't move the needle.
It's because of one of the most literal examples of survivorship bias. No living people have ever died as a result of taking some particular obviously unsafe shortcut, so they can rationalise it as OK, even though intellectually they know it's a very bad idea. Each time this unsafe shortcut kills somebody, all the living people still have no experience of dying from that shortcut because the one person who experienced the other outcome is now dead.
Close calls can help a little bit, gradually, but the effect is slow and unevenly distributed.
> it would have a greater tendency to burn itself out.
One reason I particularly point at elimination strategy (beyond the, in my opinion obviously related fact that it worked) is that zero cases has a categorically different impact than merely low numbers of cases that result from hoping a lower R-number will cause it to "burn itself out". You get to zero only one case at a time, tracking and tracing everything, getting right into the details, whereas these vague statistical approaches do not do that.
Lots of countries or regions have tried to "flatten the curve" but that's not actually a way out, it's just to buy time. Now, in this case if you bought enough time (maybe 18-24 months) you get a vaccine. But not all diseases are like that, and we could not be confident this was one.
Getting to zero is instead a (painful) permanent fix that allows you to really open up (within the country or region at zero). New Zealand's international tourist economy got a kick in the head, but its people are alive, much of everyday life is already how a lot of us in the North are hoping 2021 will be - its message this summer is "Make summer unstoppable" with small adjustments like wearing a mask on the plane, or tracking where you visited with QR code scanners - but otherwise a pretty normal vacation season, concerts, sports events and so on.
I sometimes think about this in terms of warfare. Everyone who has memories of a war survived it, and this factors into deciding whether the next war is worth it or not.
Nobody asks the people who died in the war if it was worth it.
We were mostly taught about World War I through the war poetry. They wanted our class to all memorize Wilfred Owen's poem "Dulce Et Decorum Est". I couldn't do it, got terrible marks in that class. But the Latin phrase itself sticks in your head.
Wilfred Owen did not live to see the end of that war.
It was at first astonishing to me that the same words are etched into the Arlington cemetery amphitheatre, but of course that's almost why Owen refers to them. At the time the building was constructed it would have been the thing to do - to portray death in war as a noble sacrifice.
Owen's point is that there's nothing noble about choking to death in a fog of gas, of so many dying so far from home, war is not noble or patriotic, it's horrible.
> It's because of one of the most literal examples of survivorship bias. No living people have ever died as a result of taking some particular obviously unsafe shortcut
People take something far more seriously if someone they know, especially a family member, friend, immediate colleague, etc, dies of it, compared to if the only deaths they know are stranger deaths reported in the media. So I don’t think it is true that people will ignore something unless they personally die from it, if your spouse or child or parent or best friend or boss dies from it you will take it very seriously.
I don't personally know anyone who has died from COVID. As far as I know, I don't know anyone who knows anyone who has died of it either. Probably the majority of people are in the same boat as I am. Not saying I don't take it seriously, but I'm sure I'd take it even more seriously if someone I knew died from it.
(A work colleague got sick with it, had to go to spend some time in hospital due to breathing difficulties, but has since recovered – that obviously raises the psychological impact of it for me a bit, but they live in another country, if they lived in the same country, even same metro area, as me, the psychological impact for me would be greater.)
Yeah, this was something 'interesting' to learn about people's behavior. If it had been deadlier, more people would take it more seriously. It hits a "sweet spot" where it's lethal... but not quite enough to terrify everyone into staying home. So it keeps ebbing and flowing.
What a weirdly accusatory tone. For the record, I’m staying at home and I wear a mask. Save your accusations for those who actually advocate for behavior you disagree with.
My point is entirely that the perception of risk has had a huge impact on compliance for social distancing and mask wearing. The fact that 99% of those infected survive (age dependent) has had a negative impact on compliance. If this had been a pandemic with a higher CFR, then compliance would have been even higher. I have an extremely hard time imagining there being an anti-lockdown movement for an outbreak of Ebola, for example.
1% is a huge amount of people dying. Death rate doesn't matter so much as the number of people getting it, why is why SARS with a much high death rate killed far fewer people than Covid-19.
Read what I said more carefully before replying. You’re largely reiterating what I’ve already said.
Yes, 1% CFR is a lot of deaths, which is why ~3k Americans are dying per day. But 1% of personal risk is perceived as a low risk thing, hence the low compliance.
I don't think Americans would align more to stop it if it were deadlier is my point. There would be the same stupid outcry. Look at the history of the Spanish flu. It's the same crap.
"High lethality is often associated with reduced transmissibility. Which makes sense - dead people certainly aren't going to cough on you."
The worst case I can think of is an ubiquitous animal vector (rats? mice?) that only gets a mild form of the disease but can spread it, while people fall dead all around.
Like with the plague. This is why it stuck around for centuries while causing high death rates. Without the animal transmission it would have been much more contained.
Obviously, it was made worse by people blaming cats and killing their best defense.
>> High lethality is often associated with reduced transmissibility.
I think the scariest combo would be long incubation time + transmissibility while asymptomatic + high lethality when symptoms appear. This type of virus would spread far and wide before it’s detected, and would also be very deadly.
The nasty part of coronavirus is that while you are most contagious in the first 24 hours of symptoms presenting, you are also meaningfully contagious for about 48 hours prior to symptoms appearing.
It makes me wonder how the world would cope today with a Bubonic Plague or Spanish Flu, those two I reckon would probably be more similar to your hypothetical Sci-Fi disease.
On the Spanish Flu specifically, the evidence indicates most people who died were killed by secondary bacterial infection, not the virus itself[1]. This was the result of a combination of poor hygienic conditions and lack of antibiotics. Considering that, I think what we are witnessing with SARS-CoV-2 is about what the Spanish Flu would look like today.
Bubonic Plague is still around, quite deadly if untreated, antibiotics work if given quickly enough (and are used as a preventative measure for contact persons). Large outbreaks are rare.
I've been wondering - would it be possible that something like HIV comes along, only airborne? This would be a nightmare scenario obviously, but is it possible?
Definitely possible, but I (not an expert) think unlikely. Viruses still have to contend with physics and limited resources.
For example, by “something like hiv” do you mean something that acts very slowly, but eventually kills you? That indicates a low viral reproduction rate - which means you’re spreading far fewer virus particles than something like covid, thus a low transmission rate, even if airborn.
Do you mean “attacks the immune system”? How does it get airborn, if it’s in the relatively few immune cells in the lungs? I suspect if you inhaled an aerosol of hiv particles you might catch it, but it doesn’t have a way of getting in the air.
Again, not an expert/wild speculation, but I think the risk of something fast acting, highly transmissible, and highly lethal, is more of a concern than a slow-acting lethal virus.
If the strategy is 'everybody stay at home' then it work in the same way shot gun works in eliminating cancer. It works but the cure is worse than the disease.
It’s normal here in NZ and with the exception of borders, restrictions were removed a fair while ago. The economy is considerably better off than most expected too.
However, Stats NZ national accounts manager Paul Pascoe said the effects of Covid-19 on different industries had varied “and for some industries these may persist for some time”.
The rebound was not enough to make up for the lost activity during the lockdown period, with GDP in the 12 months ended on September 30 down 2.2 per cent on the prior year.
I am certain GDP has been nobody’s primary concern in NZ during this time, but -2.2 % is not bad considering how international NZ’s economy is. For comparison, UK is at -9.6 for the same period US -2.9 with a far higher human cost.
There are many who argue against lockdowns, but I haven’t yet seen an argument for that approach with an example of how it could look (for death toll and the economy). Has any country managed both those things without a lockdown?
A hand waving “that approach could never work in X country because it’s so different there” seems the standard response to any strategy that has been proven to work.
Sweeden is one example, the death toll is still manageable and the life is pretty much still normal.
Not a country: florida, it is one of the state in the usa that has the least covid related restriction. They are doing very well. Went there myself to visit recently.
Its not hard to see why lockdown is not worth it. According to cdc, covid has very very low ifr :
It gets real dark real fast. The Post link suggests that their approach has worked, as long as you value a human life at no more than $1.1m. They are approaching 8k deaths and their approach is suggested to have added 5k to that.
“ Assume that the differential Swedish approach dampens the GDP fall this year by 1 percentage point. This represents a gain of approximately $5.6 billion. Also suppose that the approach has caused 5,000 extra deaths — a reasonable guess from comparisons with other Nordic countries. How could one estimate that loss of life in economic terms? The value of a statistical life, used by the Swedish Transport Administration in its cost-benefit analyses of investment in traffic security, is approximately $4.6 million. Using this number, the economic cost of lost lives would be as high as $22.9 billion — clearly outweighing the benefits from the smaller GDP fall. One might argue that the value of lost lives should be set much lower, as the vast majority of deaths have been among elderly people, with fewer years left to enjoy life: 89 percent of the dead in Sweden have been above 70 years of age, and 67 percent above 80. One reaches the break-even point in my calculation if one lowers the value of an average life lost to $1.12 million. For the Swedish approach to be “profitable,” the average life lost must be valued lower than that.”
That this is not some uncontrollable inevitability is the whole point. Places that were proactive have less economic harm and far less death and illness. I suppose people aren't going to change, so the ship has sailed for much of the world, but it wasn't inevitable for vast numbers of people to get infected.
As far as 1/200 being subjectively low, if something had a 1/200 chance in killing you, would you do it 5 times a day? We can answer probably not of course, because you probably wouldn't do it once a week (or you wouldn't be).
The point is, even without any precaution, they might never be infected in the first place, so probably death from covid for this specific age group is : probability of getting infected * 1/200. So even less than 1/200.
If I'm in this age group, obviously I would happily take this chance, if the alternative is lockdown/restriction.
> As far as 1/200 being subjectively low, if something had a 1/200 chance in killing you, would you do it 5 times a day?
It would probably be considerably more fun to self isolate while taking up drinking, smoking, motor biking without a helmet and a variety of other risky activities. At least those are interesting, and they are probably less risky.
That is his opinion, which I disagree. I myself would not consider it 'failed'. Sweeden total death this year is not significantly different compared to previous year.
What are you taking about? Sweden reported that this November was the deadliest in the last 100 years since the Spanish flu in 1918. Compared to Norway, Sweden has 20x more deaths from covid (Sweden 8000 vs Norway 400 deaths) and Sweden has only 2x population (10M vs 5M). And Norway has a better GDP than Sweden despite stricter lockdown policies.
Searching about I see data like yours and ones like those I include below, which show an excess. Why these differ, I don’t understand.
In your link, if you assume the death rate for the remainder of the year will remain static and calculate the end of year total (it’s roughly adding 5%) you get a number that looks like it spikes, but not hugely.
The below show a clear excess and a long tail after the spike in deaths.
A conspiracy theorist acquaintance of my sisters sent her data in our country that was wrong, same argument - look COVID-19 isn't killing anybody, it's a plot, blah bah. The raw data (weekly mortality) is published by government on a weekly basis and I just explained to my sister how to download it into Calc or Excel or whatever and see for herself.
One of the recurring things with conspiracy theorists is that they aren't in the least interested in fact checking. They're engaged in a search only for reassurance that they're correct, if you give conflicting data they keep searching but if any source will agree with them it must be right.
You probably shouldn't add only 5% based on the remaining days. Deaths stats are frequently preliminary for weeks or even a few months as reporting itself may be delayed (in particular right now if you're quarantined and a sick person passes peacefully regardless of cause what's the point of breaking quarantine to do paperwork more quickly? They aren't any more or less dead if you do the December 1st death paperwork on December 15th)
We'll see what the number end up, covid has spread since the beginning of this year, highly unlikely that in next 2 weeks suddenly the death jump significantly.
Also keep in mind that the excess death may or may not be due to covid alone.
> highly unlikely that in next 2 weeks suddenly the death jump significantly.
Is it? Cases have been spiking but deaths are going in the other direction or are flat lining. There is usually an increase in deaths about a month after covid cases go up.
Even conservative modelling predicts a lot more deaths (+50%) and less conservative models see a doubling or more.
The entire country only locked down once, starting March, reducing to milder conditions in April and totally ending (going to "Alert Level 1" which isn't the same as before COVID but it's pretty much normality in everyday life) on June 9th. But Auckland (their biggest city), locked back down after another cluster of unknown origin was detected, perhaps related to an import business, for several weeks from August, and the rest of the country was at "Alert Level 2" in that period until the first week of October.
Subsequent small outbreaks have not triggered a lockdown because their government remained confident it understood the scope of the infection although one leak got close, they asked people not to travel into central Auckland for a day or two at one point and sealed off a residential building while they tested everybody who lives there.
They anticipate continuing to have occasional small outbreaks detected, e.g. a border worker gets infected, infects a family member before a test spots it - and their plans assume they will either quickly achieve confidence they've contained the outbreak or they'll lock a region or if necessary the entire country back down to eliminate.
For example at a press conference the press basically wanted to know if the government was imagining people should prepare to pay for an extra week's accommodation on vacation in case they can't return home (obviously unaffordable to many families) but the government seemed to be more thinking about if you've left a week's cat food and instructions for a neighbour, do you have a way to tell them they need to feed your cat for an extra week? So, personal anxieties rather than population scale ones, the government can pick up a hotel bill but it can't bring your pets back to life.
Just last night on the news they announced we were actually out of recession. The bounce back has been pretty good. Tourism is still fairly impacted. Most everything else feels pretty normal.
The lockdowns were worth it IMO. Especially now we see it ravaging the rest of the world becoming more and more severe. That just feels totally foreign to me since we only experienced a very mild outbreak initially, followed by a tiny one a bit later on.
At the of the day how it is received is down to the individual. Our family is healthy and we've all kept our jobs and none of us are suffering any form of hardship. Lockdown was temporary.
Some people have lost businesses, jobs or careers and they're going to be less happy about that.
From my day to day perspective my life is very normal. I remember the level of background anxiety grew rapidly the more it spread into the community in the initial outbreak. The second and third waves around the world look increasingly terrifying.
Can you explain your preference for no-lockdown?
NZ is covid free, the economy is rebounding fast and we have had very few deaths and (relative to others) short lockdowns. Unemployment is considerably less than expected. Christmas is shaping up to be normal.
The results in NZ are only subjective if you pull some elaborate contortions, NZ has done well.
Few months lockdown is not short at all. Even then they still not allowing international visitor.
My preference is simply based on cost/benefit analysis.
I'm not opposed of covid free at all, as long as whatever method you choose doesn't cause problem that outweight the risk.
Here is some example that is not a lockdown:
Increasing health care capacity
Developing better treatment
Use more accurate test
Sweeden, florida has done very well too without lockdown. Although there is still possibility that their politician succumb to pressure and enact lockdown in the future.
Downside of lockdown: unemployment, bankruptcy, mental health issue, delayed treatment of other illness, kids can't attend in person school, etc.
You can say that all of these is not big deal. I still respect you while I disagree with you, after all its subjective preference.
>elaborate contortions
Please don't use these words just because we have different value.
You give Florida as an example. If we scaled up New Zealand's population to Florida's their total COVID-19 fatalities would be about 100. But Florida's policy approach has killed over 20 thousand people already, and shows no sign of stopping.
You list as a downside of New Zealand's approach unemployment. Scaled up, New Zealand would have about 600k unemployed people. But Florida actually has 650k. So that seems like instead of avoid unemployment, an economy devastated by pandemic but unwilling to lockdown has shrunk anyway.
So so far your cost is twenty thousand extra friends and relatives dead, and your "benefit" is fifty thousand extra unemployed.
Did you actually perform a cost/benefit analysis? I don't think you did.
>But Florida's policy approach has killed over 20 thousand people already, and shows no sign of stopping.
Keep in mind that the 20000 death number is highly inflated because it include death with covid not just due to covid. People who happen to be covid positive during the death is included in the number.
Most importantly with the current death number, i didn't say florida government handling it perfectly but I much much rather to live in this place if I have choice.
If you think its a horrible way to live then only thing i can say: to each their own.
>and shows no sign of stopping
as more and more the virus spread, more people develop natural immunity
as times go the treatment method improve
and then there is vaccine coming
>But Florida actually has 650k.
Keep in mind that unemployment number is not all solely caused by lockdown
But for sure some unemployment is caused by lockdown due to simple logic: if you don't allow business to open due to lockdown, the worker wouldn't have job.
My simple cost-benefit analysis:
The risk/cost of covid :
less than 1% death rate and mostly skewed to older population
The lockdown risk/cost:
Some unemployment, some bankruptcy, some mental health issue, some delayed treatment of other illness, kids can't attend in person school, etc
At least for me The lockdown risk/cost is much more than the risk/cost of covid
>So so far your cost is twenty thousand extra friends and relatives dead, and your "benefit" is fifty thousand extra unemployed.
More accurate example would be: 1 people I know dead due to covid, benefit : life continue as normal for the rest of people.
Pretty damn worth it to me.
> Keep in mind that the 20000 death number is highly inflated because it include death with covid not just due to covid.
Although 20 thousand people's cause of death is listed as COVID-19, about 27 thousand excess deaths occurred already in Florida, and that'll probably be closer to 30 thousand by New Year.
So, rather than 20 thousand being "highly inflated" as you propose it's likely a considerable undercount.
> But for sure some unemployment is caused by lockdown due to simple logic: if you don't allow business to open due to lockdown, the worker wouldn't have job.
Unemployment is being caused largely by the economic slowdown, and by significantly reduced footfall, driven by inability to control a pandemic.
Of course in New Zealand that's largely restricted to just one sector: International tourism, whereas in Florida their whole economy is constantly being kicked in the head by the policies you admire and will be for months to come.
>27 thousand excess deaths occurred already in Florida
Are the excess death is solely caused by covid ?
>Unemployment is being caused largely by the economic slowdown, and by significantly reduced footfall, driven by inability to control a pandemic.
I'm not saying I agree with all Florida government policies. The unemployment issue exist even without pandemic, but here I'm specifically taking about the unemployment that is caused by lockdown.
if you don't allow business to open, then some extra unemployment bound to happen. Assuming the lockdown do work, Is it worth it for a virus that have less than 1% death rate ? for me its very very not worth it. Furthermore unemployment is just one of the many of problem caused by lockdown.
> Are the excess death is solely caused by covid ?
Not all of them, I'm sure plenty of people in Florida committed suicide out of despair, drank themselves to death and so on as a result of the pandemic virus as well. It would be easy to become hopeless somewhere with tens of thousands of needless deaths while idiots cheer it on from a safe distance.
> if you don't allow business to open, then some extra unemployment bound to happen
If all your businesses are "open" but potential customers sensibly choose to reduce their exposure by staying away, unemploymentment sky-rockets anyway, as it has in Florida. Then you'd need substantial government action to prevent the worst effects of that, and of course that was never likely under Trump whereas Ardern's government in New Zealand immediately began programmes to try to prevent employers going bankrupt during Level 3 and to protect individuals from the economic impact, as well as pursuing elimination strategy for the virus itself.
As a result New Zealand was able to largely re-open and is already well into its economic recovery - aside from international tourism. They're having a pretty good summer.
Your problem is that you started with a belief you wanted to justify and then you've embarrassed yourself by pretending you've proceeded rationally when actually you were just making excuses. Just admit to people how it is, you're a selfish asshole who doesn't want to obey restrictions that keep other people safe. Just say it, if it makes you feel bad that is, after all, your problem.
> The underlying technology may have taken years, but it can be applied to new viruses as soon as the virus is sequenced.
My understanding is that a big part of why this one was so fast was that Moderna had experience digging into SARS previously, and that led them to immediately focus on the spike protein this time around. Without that prior experience I expect it would have taken longer? (But likely still pretty fast.)
As http://cis471.blogspot.com/2012/08/seeding-internet-cost-gov... lays out, the government spent $25 million on ARPAnet, the first packet switched network and the granddaddy of our current Internet. So it was actually the same figure as this grant. (There were followup investments from the government, but the whole thing was around $125 million.)
There was also heavy government censorship of the press during WWI, which suppressed early reports of the pandemic. That should be a cautionary tale to people in the present day who want more centralized control over what people can say online - the censors might not always be on your side.
>Many were increasingly of the opinion that they’d all made a big mistake in coming down from the trees in the first place. And some said that even the trees had been a bad move, and that no one should ever have left the oceans.
The internet is great, how we use it may not be.
I don't have twitter, rarely delve into comment on most news sites and Youtube. Browse and sometime comment on Reddit and here. I prefer here, less shouty.
When you are able to talk to thousands or millions of people without having to have connections, its a wonderful thing. The friction arises from a number of things; contrarians who love to argue, trolls, governments/companies who are trying to influence opinion but also people who have a genuine different opinion and are unwilling to listen to the other side.
I did enjoy the internet more when it was younger but at the same time, there was a less diverse population on it then.
Sure, and that website I made in 24 hours was only possible because of DARPA's funding of the first Internet and decades of efforts into programming languages, etc.
The point being, if a novel deadly virus was discovered tomorrow, how fast could Moderna develop a potential vaccine?
It depends complete on what kind of virus it is. All of the interesting research required to hit "print" on mRNA-1273 was already done in MERS. It would have been surprising if the vaccine didn't work.
If a new pandemic emerges from a less well understood family of viruses for which we don't have any good preclinical vaccines, it could still take decades.
Sticking the genome into synthetic mRNA isn't the rate limiting step, it's knowing to target the spike protein, inserting the stabilizing proline mutations, &c and also having experience getting safe and protective responses from a similar vaccine for a related virus.
> The question ultimately comes down to risk vs benefit. We need to get over our evolved but suboptimal instinct to avoid directly causing harm preferentially over passively allowing harm to occur. In the end, the amount of harm is all that matters. In a situation like this, delivering a vaccine as quickly as possible while maintaining sufficient safety and efficacy, there is a sweet spot somewhere that minimizes disease, death, and disruption. We want that sweet spot, even it if means delivering a vaccine that has not been tested as much as we would like. It would mean accepting more risk form the vaccine in order to reduce risk from the pandemic.
Looking at various safety standards, risk/benefit analysis is well established in the medical environment (and only there); e.g. ISO 14971 states "If the residual risk is not judged acceptable using the criteria established in the risk management plan and further risk control is not practicable, the manufacturer may gather and review data and literature to determine if the medical benefits of the intended use outweigh the residual risk."
I think that is the key quote but I believe their conclusion about balancing risks is mistaken. People don’t statistically assess risks the way actuaries do, even the most rational people don’t think like that. There’s already a significant percent of the population that believe any number of irrational things about vaccinations. Around a third of Americans aren’t planning to get the vaccine. If there are a significant number of adverse reactions convincing people to behave rationally will become even more difficult. When assessing the risk we can’t just look at the direct effects we also need to consider the effects on how the population at large will behave.
No, it took years to develop the vaccine. Luckily they started on it before they even knew whether there would be a big payoff. Otherwise we wouldn't have either the Moderna or Pfizer vaccine.
I'm generally against pharmaceutical companies charging ridiculous prices for their drugs, but we've benefited from the fact that they use this money to pursue risky research opportunities. If the chance at a big payoff wasn't there, big pharma might not have had this in the hopper. Government funding alone probably can't incentivize pharma to continue pursuing long-shot bets at their current level. Now I have to think about which option I would prefer- cheaper prescriptions or a better chance at being prepared for catastrophic events.
Probably not since January, but maybe after the phase 1 trials and the dosing schedule was figured out. To be honest, if it doesn't come out that they were using it off the books, either they're suckers or we are.
Would it even be a problem if they did? Like presumably people are generally free to do things to themselves. If they self-administered and they were allowed to consume the resource (e.g., it wasn't theft) who was harmed?
It could be a good thing to leak it to the press. The press would feign a scandal but it would actually have the effect of showing people that they believe in their product and only a slap on the wrist would actually happen (if anything).
> To be honest, if it doesn't come out that they were using it off the books, either they're suckers or we are.
Considering high-level officials in the government apparently never received the vaccine, I would be surprised if the people involved in the research took the vaccine.
Then again, maybe secret was kept extremely well. My intuition is, if POTUS knew about it, he would have been telegraphing such on twitter back in the summer months.
A corporate gifting of one to every rank and file employee like some sort of morally questionable bonus is a bit different from, what I assume GP meant, folks in the lab actually working on it pricking themselves to test, or because they believe in it, can't resist, etc.
> If you've got elderly loved ones you want to keep safe, you'd need to vaccinate them, not yourself.
If the vaccine substantially reduces viral load, and degree and period of contagiousness for those who receive it, as well as reducing the risk of illness (which AFAIK it does, while falling short of sterilizing immunity), and you are the elderly loved ones main interface to the outside world, getting vaccinated on top of other precautions provides a real benefit.
OTOH, if you have to choose one to be vaccinated, it's them, not you. If you do this for lots of elderly family members, getting yourself vaccinated may be better than getting any one of them vaccinated, though. And, of course, of you are doing an off the books pre-approval use of the vaccine, accepting the risk of unexpected side effects for yourself may be more reasonable than imposing them on, or even suggesting them to, someone else who may be in a more fragile state.
There's a strong social benefit too. Being able to more comfortably spend time with friends and family you care about, even if they can't be vaccinated yet, seems worthwhile in itself. There's also the related consideration for dating, etc.
Unfortunately not. Being vaccinated doesn't stop you from having and transmitting the virus, only from getting sick. It won't be safe for you to see your friends until they have it too.
> He said the findings reflect an impact on blocking transmission and are very encouraging, hinting at mucosal immunity. "The data aren't conclusive but support this key benefit," he said.
Of course, if in the end vaccines don't prevent transmission, then they don't prevent transmission. But we don't know that they don't do that.
It's not irrelevant though. I know someone who is 39, perfectly healthy and nearly died. He now has long covid. I'm sure all of the people under fifty who died would have loved to have had the vaccine.
What's the downside though (if you figure it's safe and effective)? Even though you still can't go anywhere and have to wear a mask, why not reduce your risk to 0? Even if you only have a mild case and there's no long term damage, being not sick is still a lot more fun than being sick.
They probably could have finagled themselves into a trial.
I know a friend that got the Moderna vaccine that way. Technically, it was double blind, but it is fairly obvious whether you got the real vaccine or not.
What this class of vaccine does is make a bunch of foreign proteins for your immune system to attack in your arm without actually infecting you with the disease. So you get inflammation and soreness at the injection site, and this is not from the physics of having an injection. The placebo arm injects with a saline solution, so there's no immune response, and you miss those symptoms.
Do you think people could perceive having "false" inflammation? I'm thinking that if during the double blind trial they told those not getting the real dose that they should expect inflammation that many of them would believe they're having some form of inflammation.
It might have been the trial for a different vaccine; I think it was the one someone on this site was participating in? But in that trial, the control was another proven vaccine for something most people don't commonly get vaccinated for.
That's what I thought, but my effects were mild compared to what I've heard other people reporting. Either I got milder side-effects because I'm young, or I'm fooling myself.
2) My reading of the 2018 (best I found sorry) mortality table for 35-44 age group would put death by covid as the 5th leading cause of death. Just between suicide (7521) and homicide (3304).
For every person who dies of COVID, nineteen people are hospitalized. Eighteen of those will have permanent heart damage. Ten will have permanent lung damage. Three will have strokes. Two will have neurological damage leading to permanent muscular disability. Two will have neurological damage leading to cognitive impairment.
Don't be afraid of covid killing you. Be afraid of it turning you into a mentally disabled cripple who can't catch his breath until you die of heart failure twenty years before your time.
Edit: Oh and just for kicks, there's recent evidence it causes erectile dysfunction too.
I often wonder how many people actually believe things like this, versus are willing to say them loudly in the hopes that they'll make others take the virus more seriously. Because none of this is remotely evidence-based.
It's well known that respiratory diseases cause permanent damage. We see it with flu and we see it with covid-19. "Damage" covers a huge range though.
In June estimates were that 1 in 5 people who needed intensive care for covid were left with permanent damage.
> People infected with the coronavirus may be left with permanent lung damage. Doctors are reporting growing numbers of people who still have breathlessness and coughing months after falling ill with covid-19, and whose chest scans show evidence of irreversible lung scarring.
> The numbers of people affected aren’t yet known, but estimates are as high as one in five of those who needed intensive care treatment for covid-19. Permanent damage is sometimes seen after other kinds of chest infections that can cause similar lung inflammation to the coronavirus, such as flu and pneumonia.
> In a study in Italy, which was one of the first European countries to be hit by the coronavirus, doctors are scanning the lungs of people three months after they fell ill. Although the full results aren’t yet in, Paolo Spagnolo at the University Hospital of Padua estimates that 15 to 20 per cent of those treated in intensive care at his hospital for covid-19 have scarring. “We have to be prepared in the future to manage these patients.”
You seem so confident, but cite nothing (just like the comment you are referring to). However, I do note that all the symptoms noted in the comment above are actual symptoms found in survivors of severe COVID. I'm not sure about the proportions though, but is it a stretch to believe that patients who are hospitalized (by definition, severely impacted by COVID) very often have long-term damage?
Yes. The question is not whether bad health outcomes exist, only the truly ignorant believe COVID is a total hoax. The question is whether COVID is significantly worse than the influenza, rhino, and corona viruses we generally get year-round. The answer, is resoundingly yes. COVID is much worse in terms of the short-term and long-term sequelae both in terms of the range of "bad health outcome[s]" and in terms of the likelihood that an infected person will have one of these "bad health outcome[s]".
I won't be surprised if Covid ends up being slightly more or slightly less correlated with post-infection issues, but we have seen no credible evidence of this at all, much less evidence that we should worry Covid turns you into a "mentally-challenged cripple."
Also the death rate as a catchall metric completely ignores people who here in absolutely critical, life-or-death condition but were only saved from death by incredible medical intervention and/or just pure luck.
Another terrible metric comes in here, money.
What does the annual flu season cost versus the covid cost?
Money is a bad metric but it does boil things down to one measure. I’m sure these aren’t measured the same way but the effects haven’t been similar. Flu $90b per year versus the covid cost of $16t.
> Flu $90b per year versus the covid cost of $16t.
I mean that miiiight have something to do with the fact that we basically ignore the flu despite tens of thousands of deaths every year. Whereas with Covid we collectively decided to shut down the entire world.
Yes, and why were the shutdowns done? If you compare what happens with uncontrolled covid spread to a those of a flu season, they aren’t really all that similar. Even with the lockdowns, the deaths have been considerably more than tens of thousands.
Wrong. First, you have no uncontrolled covid spread to compare to. You are actually comparing tightly locked down COVID spread to a normal flu season. And COVID is still killing a lot more people. The closest example for an "uncontrolled covid spread" would be Bergamo in Jan-Mar 2020. Is that what you want repeated world-wide? The death rate there was astronomical.
So remember that’s tens of thousands of annual deaths with a vaccine. And what good have lockdowns really done? The virus seems to spread regardless. Look at all those European countries the US was compared to during the summer as an example of how to “do it right.” Not sitting so pretty right now...
The lockdowns in Europe worked. Full stop. Case rates dropped dramatically.
Some of those countries are "not sitting pretty right now" because they ended their lockdowns.
The answer is not "lockdowns don't really do any good." The answer is "don't prematurely end your lockdowns." Now that can be burdensome. You can do a middle ground (limited re-opening). That works too, but you have to be very careful and keep a close eye on case numbers and shut down totally as soon as cases ramp up. California tried to do that in the latest surge, but was a little late in implementing the newly stringent measures and even further So. Cal. "resisted" the newly stringent measures and are now suffering mightily.
I don’t think any European country has completely lifted their lockdown restrictions. All of it is a “limited re-opening.” Perhaps respiratory viruses spread much more effectively in the winter versus the summer? Maybe that’s it? Nah, it must be that everyone in Europe has perfect hygiene and practiced social distancing perfectly in the summer and they’ve all forgotten how to do those things now.
> I don’t think any European country has completely lifted their lockdown restrictions.
True
>All of it is a “limited re-opening.”
Yes, but the issue is how limited was the limited re-opening. I live in the U.S., but ALL of my colleagues are in Europe. It's anecdotal, but my understanding is that the re-openings throughout EU were quite closer to the "unlimited" side than the "total lockdown" side of the spectrum.
>Perhaps respiratory viruses spread much more effectively in the winter versus the summer
The presence of an additional explanatory factor does not prove the absence of an alternative explanatory factor. They could both be true, and almost certainly are true. That is: lockdowns work; without lockdowns, you have Bergamo in Jan-Mar 2020 (mass death); COVID spreads better in winter.
Well, (a) obviously working age extends well past 40s, generally to mid-late 60s (and higher in some countries). (b) people in their 30s and 40s often have older friends and relatives, who they are disinclined to kill.
I'm 35, and am not super-worried about dying of covid; it's certainly possible, but not hugely likely. However, I'm extremely worried about being a vector.
I am very concerned that moderna is such an incredibly inexperienced company when it comes to actually delivering products. Companies like Pfizer and Astra etc have lots of infrastructure for manufacturing and logistics, as they’ve been making drugs for years. Moderna hasn’t ever released a product before, and now we need them to successfully make hundreds of millions or billions of doses of it very quickly? I have every confidence that the drug itself is safe and effective, but I fear that they won’t be able to deliver on the quantities required.
McKesson is handling distribution for Moderna, and one of the main goals of Operation Warp Speed was to ramp up production using companies who are good at it so the vaccine developers wouldn't necessarily have to do large scale manufacturing themselves.
Suppose an mRNA vaccine is developed for some virus, but it fails to clear phase 1 safety testing.
Question: what would be the likely reasons for that? In particular, is it almost certainly going to be due to whatever carries the mRNA, or could the mRNA itself be the problem?
If it is the carrier in which potential safety issues lie, does that mean that once we have one successful safe mRNA vaccine for virus A, then when some new virus B comes along an mRNA vaccine for B that uses the same carrier is going to be as safe as the vaccine for virus A?
If so, does that mean for future new viruses, the mRNA approach will let us go right into effectiveness testing, skipping phase 1 safety testing?
Phase one is about dosage at least as much as safety. The most likely reason to fail is probably that it doesn't produce an immune response at any reasonable dosage.
Is there any risk of a "doesn't produce immune response" failure that would make it unsafe to start giving to healthcare workers immediately? Could it make later vaccines ineffective?
I'm sure that it would ruin the data for later vaccines, but if high-risk people just take each new vaccine as it starts trials, their data doesn't have to count towards the actual trial.
Don't downplay the safety. Phase 1 can fail because of lack of immune response OR safety concerns. Phase 2 and 3 trials are also about safety, and both of them somewhat often fail because of safety issues.
A vaccine can make a disease worse by priming the immune system to overreact and attack the entire body when a single cell is infected.
The more we know about a vaccine the more confident we are. The flu vaccine is changed every year without long safety studies: we have learned enough about how people response to the flu vaccines in use to not need them anymore. When the same process is used to make a non-flu vaccine though we still have to start over because there isn't any way to be sure.
You are quickly getting beyond my area of knowledge though. I didn't answer all of your questions because I don't know.
Dengue fever is a strange and terrible disease where -- unlike most infectious diseases! -- contracting it once can make future infections worse through autoimmune mechanisms (if I remember correctly, you typically become immune to the particular strain that caused the first infection, but may become more susceptible to severe reactions from a later infection involving a different strain). Apparently the Dengvaxia vaccine, while effective at reducing the chance of dengue infections, also has an effect similar to surviving an infection: it increases the chance that an infection will result in severe disease. That makes it a more complicated question whether it's a good health intervention in particular circumstances, and in the Philippines there was a big scandal where a childhood immunization program using it may have reduced the total number of people who contracted dengue, but also increased the severity of the worst cases.
To my knowledge the pathogens that cause COVID-19 and dengue fever are extremely different, but it seems logically possible that there could be a COVID vaccine that greatly reduced people's chance of getting sick at all, while also increasing the chances of severe symptoms for those people who did get sick.
In therory, the mRNA vaccines should be extremely safe, as they are so specific and only require a carrier but no other substances in the vaccine. In practise, you still need to test. There is always a small risk of something unexpected happening. Like the vaccine from Australia which has been completely abandoned - not sure whether it also was mRNA or some other kind of vaccine. It didn't cause any health problem, but the vaccinated people were tested as HIV-positive. Of course they were not, but the vaccination caused those false positive. So while no direct heahlt impact, it is quite a disaster if one couldn't test people for HIV any more.
> So while no direct heahlt impact, it is quite a disaster if one couldn't test people for HIV any more.
It only invalidated certain types of HIV tests. The impact would be that some subset of existing HIV tests would have to be abandoned. That would impose a cost on the health system.
The real issue is that there were other vaccines being developed that were equally effective but which did not have this drawback. If this was the only vaccine available, the health system would have worn the burden of changing HIV test regimes; given several other effective vaccines are becoming available, it wasn't clear that the cost of imposing massive changes on HIV testing regimes was justified.
There are three options, the mRNA "carrier", such as the lipid particle, the mRNA itself, and of course the protein product.
The first part is hard to guess without knowing what's in those delivery methods.
mRNA, or RNA in general, can form secondary structures which in theory could affect the the cell machinery. Depending on the details this could produce side effects to the cells that take up the mRNA. This would probably be localized and a strong secondary structure may inhibit translation also, rendering the vaccine ineffective. This can be checked in silico and in vitro during design to some certainty.
The protein product I would guess is the most likely to cause problems. Essentially you can encode any protein in mRNA, so you could make the cells that take it in produce snake poison, for example, if you wanted to. Depending on how the virus protein is modified, and how it reacts with the cells/body when present apart from the rest of the virus it assembles with could bring all kinds of side effects. The severity probably depends on what exactly it interacts with, and if it's only local or it gets into the bloodstream etc.
Much of the danger of vaccine development is the possibility of activating antibody response to an off-target cell that expresses the same feature the vaccine is expressing. You can't really find those reliably without human trials.
Does anyone know the specific differences between the Pfizer and Moderna vaccines? I know the quoted reason is that its something to do with the structure of the delivery method, the lipid nanoparticles. And I've seen news articles saying that this information is proprietary and won't be released. Is that really an acceptable excuse for the first mRNA vaccine to be used on a massive scale and with about 6 months of trials?
I think this information should be made open so that other countries/companies can produce vaccines with the higher temperature requirement, not to mention that the public should know these differences and why they exist. There's gotta be more factories that have the necessary equipment, but the plans just aren't available.
On a related note, the fast development of a COVID vaccine seems to have triggered a sense of techno-optimism in certain bloggers / commentators. Here’s a recent summary by Noah Smith on the topic: https://noahpinion.substack.com/p/techno-optimism-roundup
All correct. But also, disturbingly Utilitarian. Release vaccines before they are tested, and withdraw those that cause more deaths than they save? Trading lives for lives, coldly.
There are costs to calculated Utilitarianism. The damage to public confidence in vaccines springs to mind. If a vaccine is provably killing 1% of those receiving it, yet saving the lives of 2% (and more once herd immunity is reached) it may raise some alarmist criticism (to say the least) over the safety and advisability of getting vaccinated. Making it harder to convince the public to get vaccinated at all.
Other costs are, mis-estimating the ultimate death toll may lead to killing more up front than was strictly necessary. Or the vaccine may have side effects down the road, shortening lives or diminishing quality of life (sterilization? memory loss? immune system compromises?).
Unless all the costs are factored in, Utilitarianism become a guess, and can be used to serve profit or social agendas. The law of unintended consequences will loom large.
> There are costs to calculated Utilitarianism. The damage to public confidence in vaccines springs to mind. If a vaccine is provably killing 1% of those receiving it, yet saving the lives of 2% (and more once herd immunity is reached) it may raise some alarmist criticism (to say the least) over the safety and advisability of getting vaccinated. Making it harder to convince the public to get vaccinated at all.
If that can already be calculated, calculated utilitarianism could take it into account.
2 main comments:
1) your example of 1% death rate would be detected very early in a rollout, and would represent something akin to a 10000x worse vaccine outcome that has ever been experienced. The worst vaccine ever is generally regarded as causing 1 in 10,000 narcolepsy.
2) the word "approved" is misleading. Of you change this to say "banned" or "not banned", this reads very differently. The requirement to ban everyone from taking a vaccine in order to mitigate some extreme long tail event and maintain public confidence is hard to justify on utilitarian grounds, but pretty much any other ethical framework.
Not sure what the point was you were going to make, but the mRNA technology is a big step in the direction of being able to address medical problems like writing a software. For a long time, pharmaceuticals were create in a trial and error process. It took science a long time to be able to reliably predict the outcome of chemical reactions, if we are talking about complex organic chemistry. I was working a very little bit on that in the mid-90ies. One very naive program I implemented was trying to predict the toxidity of a random chemical by its formula. We have come far from that. But with the mRNA technology, they could design their vaccine on a computer, also the production of the mRNA is highly automatized, so no experimenting in how to create it.
Developing the mRNA technology was of course decades of research, but now it is ready to be used. It also helped, that the SARS-virus was very well researched, so like with software, it the vaccine wasn't created "from scratch". It used the knowledge already present about these viruses. This means, while you might not get a vaccine against a random virus in two days (no HIV vaccine available yet), adjusting the vaccine for slight variations of the SARS-cov-2 virus, should be a very quick process.
You're being downvoted but the point is valid. To say that this was built in two days is to completely ignore the near decade of investment into mrna vaccines. Total nonsense.
That's not relevant. The point is that Moderna had a low-latency solution when the moment showed itself. It isn't that it's easy. It offers some thinking that their technology is revolutionary and that perhaps we need to revisit our calculations to see if the risk/reward means we should attempt earlier roll out.
We know, this time with hindsight, that it would have saved hundreds of thousands of lives and billions of dollars if we'd used their product on day 3.
Can we develop a protocol that can tell us that so we can use this tech on day 10 next time? Then we can save those lives.
> if the risk/reward means we should attempt earlier roll out
you still need to make sure the vaccine actually works in trials and has no severe side effects. It takes one, and only one minor vaccine scandal to completely blow the trust of the public in public health.
There is no linear risk/reward when it comes to vaccines. You need to be incredibly confident that they are safe or else you're going to screw yourself possibly for decades.
Sure, but we have experimental drug programs. People will sign up for challenge trials. We don't do it for the same reason IBM doesn't end up making the iPhone: risk aversion is really strong. If trust in the public were a thing the HHS were interested in they wouldn't have lied to the public about masks.
They're so far off the claim it's embarrassing they even said it. They couldn't write 1% of Twitter in a weekend.
Twitter circa 2006, they could clone the basics of it. And only because someone else already showed them what to do so they don't have to burn much time thinking very much or go through many learning iterations.
The article say that they spent a decade of research on mRNA vaccines before. That was obviously well before anybody knew about SARS-CoV-2/COVID-19. Does this mean that the research basically was about creating sort of like a "template" vaccine that can then be specialised or programmed with the specifics of the thing you're trying to vaccinate against?
The goal is to take someone with cancer, and then create a vaccine for the exact cancer mutation that person has. this would be a custom one-off vaccine that wouldn't work for anyone else because their cancer is different in some way. I don't know if this will work, but it would be a great improvement to cancer treatment if it does.
> Does this mean that the research basically was about creating sort of like a "template" vaccine that can then be specialised or programmed with the specifics of the thing you're trying to vaccinate against?
That may (or may not) have been the effect (at least within a narrow family of similar viruses), and is definitely something they market about their “mRNA platform”, but their immediately-previous mRNA vaccine work which was ongoing when they shifted to SARS-CoV-2, was specifically directed at MERS-CoV, another very similar betacoronavirus of significant public health impact (though a lot less widespread than SARS-CoV-2 has become.)
None of those came to market. Many did make it through trials. This is more about pushing this as a first onto the market so pharma companies can finally prove they're safe, and then making a shit ton of money on more vaccines after.
I think the title alone might be a bit misleading, I'd rather state it as "it tooks two days to develop a vaccine candidate". The mRNA vaccine method does mean that you can design a vaccine this quickly, just based on the sequence and some general knowledge about the virus. But what you don't from this are safety and efficacy, you still have to determine those the hard way. Which the article of course also mentions at length.
As far as I know Moderna and Biontech tried different variants of their vaccine. And to determine how well those work you have to do some animal experiments, and that is always much slower than designing and synthesizing mRNA sequences.
The mRNA vaccines were the fastest ones, and they worked better than expected. So I think there is a lot of promise in the technology, but further speedups are hard because they're in the clinical study part.
Yes. We need accelerated testing. In the case of a pandemic, we need to make better use of volunteers. I believe that as the history of this one is reckoned with, one of the more interesting moral failures to be acknowledged will be the failure to utilize challenge testing protocols with willing volunteers (give them the vaccine and then deliberately expose them to the virus. It is a calculated risk.)
Earlier phases could have been accelerated as well. For mRNA vaccines, deleterious effects are unlikely, inefficacy is the likeliest problem. It might be possible to be challenge testing (highly informed) volunteers within a week of a novel virus being isolated.
On a similar note, national stockpiles of RT-PCR machines and reagents would allow widespread testing within the same week.
If I’m right, these indicate moral failures deeply embedded within our political and medical systems. Better luck next time.
> In the case of a pandemic, we need to make better use of volunteers.
You’d run the risk of have a non-representative sample and wrongly estimating the effectiveness of the vaccine as well as possibly missing side effects.
1daysooner.org lists almost 40,000 volunteers, and that's without anyone official even asking for them. And you need far fewer subjects in a challenge trial than a normal trial.
You'd ask. I recall seeing multiple human interest stories about people who were eager to volunteer for challenge trials. I believe challenge trials are how the original vaccines were tested in the earlier 20th century prior to contemporary developments in medical ethics.
And you'll get volunteers. It's a rational decision for effective altruism. Say you face a 1% chance of death but a 50% chance of substantially contributing to saving a million lives. If that's technically possible, highly informed people should have the opportunity to make that choice.
I believe some of the earliest challenge testers were the developers of the drug themselves.
No, you don't, because you're infecting them on purpose. It's safe to assume that an extraordinarily high percentage of them would be infected if they were on a placebo leg of the trial.
Just curious -- would it be that much harder to develop a vaccine that was itself contagious? Recipients would expel the vaccine in their own respiration?
There is a vaccine against polio that can infect and immunize others. It uses a live polio virus genetically modified to not cause severe disease.
"The OPV is less expensive and easier to administer, and can spread immunity beyond the person vaccinated, creating contact immunity. It has been the predominant vaccine used. However, under conditions of long-term vaccine virus circulation in under-vaccinated populations, mutations can reactivate the virus..."
Interesting, like a fully engineered virus with the same spike proteins, but none of the "bad stuff"? Seems tricky, I think in order to be contagious, it needs to replicate, which is part of what makes viruses so harmful, right? Even if you can make it harmless, replicating means mutations will happen, so that's an interesting new kind of risk to take.
I had the same idea and was convinced by a biologist, that his is a very bad idea. To be able to spread, this vaccine-virus needs to infect the people vaccinated. Any infection is dangerous, as it means the virus is multiplying in your body until the immune system hopefully takes hold of it. What happens if it doesn't? This happens with traditional vaccines all the time, but the consequence is only that you are not acquiring immunity, no other harm done.
The other point is, you have made a completely new human-transmissable virus. How do you reliably prevent it from mutating into something more dangerous?
Interesting. That's not a vaccine anymore that's a strain of SARS-CoV-2 that's never produces symptoms, but is still similar enough to the original to prime the immune system. Presumably it would out compete the original in a Darwinian sense, because people who caught it would never get sick and stay home.
Risky, though, because if it turns out to be less benign than we thought - or mutates in such a way as to become lethal - we've just started a second pandemic.
There are these 2 quotes from the article that I think are a little too "handwavy" over potential real problems for the future:
> Since the platform itself is pre-tested, we won’t need to do months of testing before distribution. Still, we may need to do some testing on the specific vaccine. Perhaps much of this testing can be done with computer modeling, and some with animal testing.
and
> The question ultimately comes down to risk vs benefit. We need to get over our evolved but suboptimal instinct to avoid directly causing harm preferentially over passively allowing harm to occur. In the end, the amount of harm is all that matters. In a situation like this, delivering a vaccine as quickly as possible while maintaining sufficient safety and efficacy, there is a sweet spot somewhere that minimizes disease, death, and disruption. We want that sweet spot, even it if means delivering a vaccine that has not been tested as much as we would like. It would mean accepting more risk form the vaccine in order to reduce risk from the pandemic.
Think of the crazy amount (highlight on the crazy) of opposition you have to vaccines now. Imagine if you get one vaccine with just a slightly higher amount of negative reactions, and even a few deaths that were clearly vaccine-caused, due to rushing the approval process. You will have set back public health decades.
Look at covid: its fatality rate is actually quite low, well well below 1%. If we give the vaccine to everyone, you need to have extremely low adverse reactions for it to be a net positive because we're giving it to so many people.
I feel that these types of articles that argue "We need to get over our fundamental human irrationality" are pointless, because we are, after all, human.
and yet we're already seeing people who've gotten this vaccine who had allergic reactions, enough to need epinephrine. A member of the medical staff in a hospital in Tennessee fainted on camera after getting the vaccine.
60 Minutes did a segment in 1979 on the failed Swing Flu vaccine that didn't build protection for most, and that left many with long term paralysis. Some of them went back to normal after a few months, both there were enough that lost motor control that they had a class action lawsuit.
The fact that all the pharma companies in this release are immune from civil liability, and the FDA is also immune from civil liability, does not bode well for confidence.
Rationality can be induced if the vaccine is highly effective. If I get my family vaccinated and learn that the neighbors died due to the disease, it will be common wisdom that they died due to poor decision making.
> it will be common wisdom that they died due to poor decision making
so when, for example, someone gets raped after a night out while intoxicated or dies due to alcohol overdose after joining a frat...is the socially acceptable response now "poor decision, didn't assess risk correctly."?
The problem is one of medical ethics in an unequal society. The problem is that there's a sum of money for which I would have taken the risk and got a vaccine in January and had exposure to the disease in February.
Everyone in society would have been better off if I had been permitted that. America could have paid me and 49 others a million dollars each and come out wayyy ahead (since direct exposure tests will yield results way faster). Then a 3 month safety protocol and we're off to the races.
But I can make that choice because I am comfortably above subsistence. If I do it, you know it's because it's a combination of bravado, bragging rights, and this money I could survive without.
But if you actually allow the market to price this, the real price for the tester is approximately $10 in sub-Saharan Africa, and we know he's on below subsistence and is really trading his body for another few days of life. We find that doing this is abhorrent.
An interesting effect that inequality prevents us from Pareto optimal actions and improving the human race as a whole.
1. Run challenge trials, but don't pay participants in money. Talk up the danger and risk, and publicize the heroism of the people who volunteer. Make a spectacle of it. If you ask for fifty heroes, is there any doubt that you'd get them?
2. Pay participants, but impose a minimum price they need to be paid in order to assuage people's squeamishness. That hypothetical guy in sub-Saharan Africa might be exploited at $10, but if he's getting paid $1,000,000 then he has practically won the lottery.
Either of these would be a big improvement over the status quo, where challenge trials aren't run at all and countless people die because of it.
Meant to be a summary of the current state-of-the-art in medical ethics not in my personal view of the world (which goes so far as to allow non-fatal organ sales). You can rest assured I neither care about poor people more than other people nor do I wish to infantilize them.
I'm not a virologist but this is clickbait I think, it does not take long to synthesis fragments of the spike protein for a traditional vaccine either or program the rhinovirus vector in a more modern vaccine. I don't think that really is the bottleneck. You still need a LOT of testing as the viral antigen you are trying to vaccinate against can have similarities to human proteins for example, and the antigen might simply be a bad antigen for immunization - and this requires a lot of testing and studies.
The normal yearly influenza vaccines are also fast for example because they are well known platforms and also the antigens repeat historically and are thus (relatively) well tested.
I guess my point is that the problem of the vector to get the antigen in contact with the immune system is orthogonal to the problem of selecting the antigen for overall cross reactivity and efficiency and the latter is still a difficult and timeconsuming problem.
> They identified the sequence for the spike protein, plugged that into their vaccine platform, and voila – an mRNA vaccine against the SARS-CoV-2 virus.
A COMPUTER took two days to develop the vaccine. Think about that.
I think the key would be provable lack of ill-effects. With that we could start immediately using a kind of bandit testing to try and phase out different tweaks until finding the perfect one.
I think most importantly of all it seems that this wasn’t a very hard problem to solve, relatively speaking. Like we could throw all the scientists all over the world who worked on this at cancer and there won’t be a cure for cancer a year from now. At least I don’t think. Nonetheless I remain impressed and salute any and all scientists who either did the work or paved the way.
But this is a very exciting and important development. Akin to a moon landing.
How many diseases will be treatable or curable in the near future with this technology? Do any cancers have characteristics that can be used to direct our immune systems to go after them with this technology? I suspect a few might.
I don't know how Moderna was made, but the Pfizer vaccine is a modified spike protein: they use two edits to lock it in a pre-fusion conformation. Maybe this is easy to model in software, but I suspect that does take a little bit of trial and error to confirm it works in vitro too.
That's great. Well, if they're in at all between Christmas and New Year maybe they can quickly sort the common cold out. Then full steam ahead in January and they should have all the plagues of humanity pretty much wrapped up by Easter?
If I came across this article on facebook or something, I wouldn't trust it because I've never heard of the source (and, to be honest, I'm kind of judgy of the old design). How do you determine its credibility?
I'm concerned about the long-term effects of taking these mRNA vaccines. Have there been any studies? Is it true that you may need to take the vaccine more than once?
Big pharma companies have wanted mRNA vaccines for years. Others have been developed and even gone through trails that never got approved for markets.
There are also trials for therapeutics such as inhaled steroids; something doctors in certain regions have been prescribing off-label for months and claim to have very high success rates. Yet organizations like the NIH are saying they shouldn't be used until the trials/studies are done... and they've been saying that since August.
Honestly, I'd rather more effort be put into seeing if existing therapeutics can be used to reduce the effects of moderate/severe COIVD.
Let's face it. The drug companies got millions just to attempt to develop these vaccines, many of those attempts which will be failures. They don't care. They already have tax payer money from countries all around the world. This is a push to the first mRNA vaccine out, so the Gavi Health Alliance can start pushing more of them.
There is a huge money incentive we're ignoring. It's not on this particular vaccine; it's on all the future vaccines--some which have already been developed and never made it through all their trails/approved--and the billions they stand to make from them.
A vaccine reduces the effects of moderate/severe Covid to zero. All other treatments mean at best time off of what I want to be doing while I'm treated. That is at best, the most likey case is you still get the bad side effects - including long-covid (whatever that is, science is still working that out), just a bit reduced. I'll take zero effects.
There are many working on HIV vaccines. The virus mutates so fast that all previous attempts have failed. I wish them luck, but I'm not confident that it is possible. Time will tell.
I don't think that's the issue. With any virus, your immune system grows countermeasures exponentially (memory t-cells, antibodies, protein complements) to stop it. These stick around after the virus is gone. It's an immune system "memory"
In another infection, your cells still get infected, but the infection is just stopped very quickly. HIV has inscription and reverse transcription enzymes in it, so it can actually glue its sequence into your DNA. It changes your DNA enough to replicate it, but not enough that your cells change their structure so your immune system can't recognize them as infected (and those changes can cause your immune system to fail over time: AIDS).
Even if your body is primed to deal with HIV infections, if the infection happens, it's already too late.
I'm not sure who antiviral drugs like PREP work, but you'd need something like that permanently in your system.
India's death rate has been much lower than the US. Part of this is because they're already doing widespread cholecalciferol roll-out.
If cholecalciferol is not on 2021's CDCs/FDA/AMA number one recommendation list for pre-Covid control, I will have considered the AMA a complete and utter failure in the united states.
> We didn’t understand early on what a major risk factor obesity was. … It’s not until more recently that we’ve realized the devastating impact of obesity, particularly in younger people,” says Anne Dixon, a physician-scientist who studies obesity and lung disease at the University of Vermont. That “may be one reason for the devastating impact of COVID-19 in the United States, where 40% of adults are obese.”
First of all it seems unlikely people in India don't get enough vitamin D, it is a lot further to the south and inside the area that should have enough sun year round.
I don't think you can compare death rates in India and USA, the healthcare and accountability is just way different. Even though it is not great for the poorest ~50% in USA, it is really not good for the poorest ~90% in India. Those numbers are made up, but meant to illustrate that real healthcare in India is mostly for the wealthy.
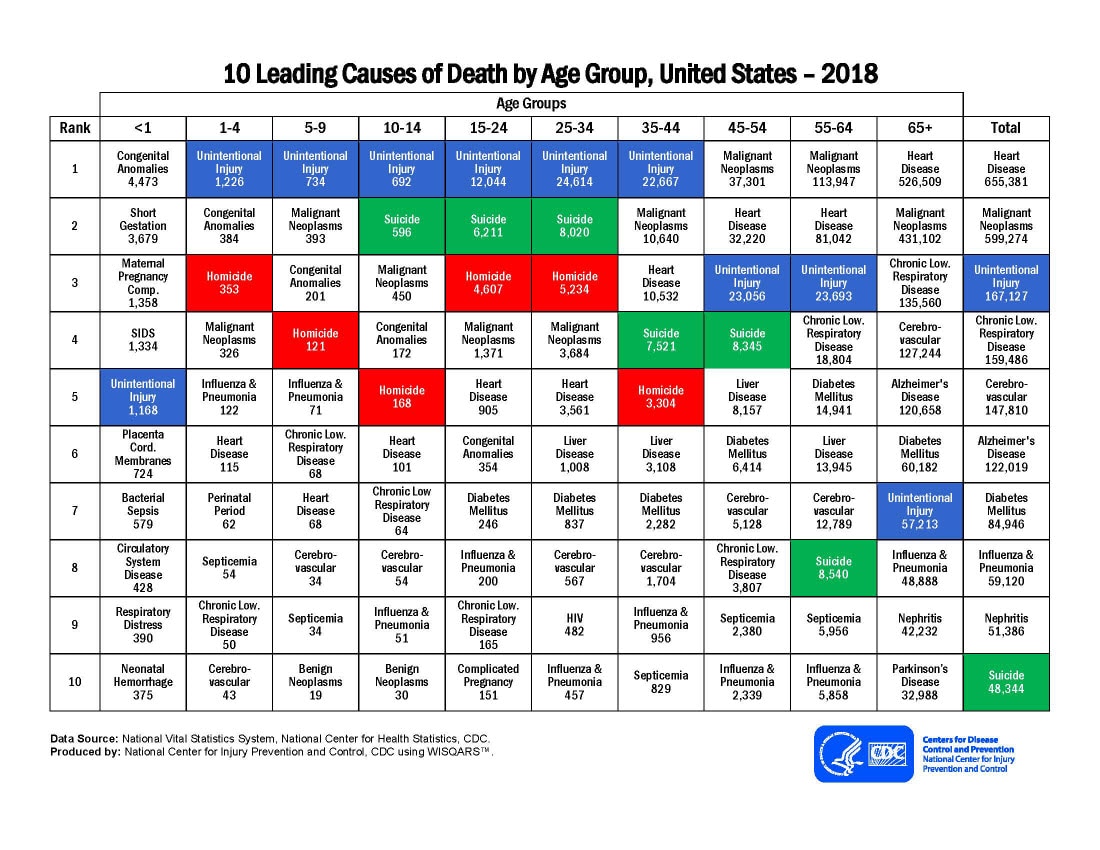{kind=link}
My brother is a doctor and he got his Pfizer shot yesterday. Less than one year has passed since the first case in the USA. I consider this one of the great accomplishments of science. It will go unnoticed by many idiots on social media but it is an amazing achievement by all the scientists and doctors involved.