> the immune system has an array of other defenses... including antibodies that attack other parts of the virus, and, importantly, T-cells that attack the infected cells the virus hijacks in order to replicate. “What we’re seeing is that these variants don’t seem to affect T-cell immunity all that much and they [the T-cells] seem to be as effective in recognizing these variants as they do the original virus”
People with healthy immune systems, who have been exposed to SARS1 and other coronaviruses, have active T-cell defenses which recognize SARS-Cov-2 even without a vaccine.
> ..some people who have not been exposed to SARS-CoV-2 have preexisting reactivity to SARS-CoV-2 sequences ..previous exposure to widely circulating common cold coronaviruses might be involved .. preexisting reactivity against SARS-CoV-2 comes from memory T cells and that cross-reactive T cells can specifically recognize a SARS-CoV-2 epitope as well as the homologous epitope from a common cold coronavirus,https://science.sciencemag.org/content/370/6512/89 (Oct 2020)
I have done my PhD on T cell activation. The persistent focus of the media and even some of the science community on Antibody induced immunity was completely beyond me. T cells were largely simply ignored even though they play such a crucial role in the body’s immune response.
Antibodies seem to be a concept much easier to grasp. Maybe we should call T cells "Police Cells or "Anti-Cells" instead. You know, some marketing might help...
T cell activation is readily misunderstood even among some cell biologists. There's a lot of people in life science academia who desperately need to update their knowledge about the recent discoveries in Immunology.
Are vaccines necessary for someone who has had covid? If it was absolutely necessary to prioritise those who don’t have any immunity at all, is there a test that can help identify with that?
>The test is administered via blood draw. T-cell DNA is then extracted and sequenced with Microsoft's artificial intelligence, mapping out the immune system's "massive black box" data into navigable science, researchers say.
> We provide practical hints and tips on basic cellular and molecular techniques for handling primary human T cells. We hope that this guide will serve as a reference point to evaluate, discuss, and improve current practices in T cell culturing and manipulation.
> Killer T Cell is loud, obnoxious, and quick-tempered, resulting in rivalries with many cells. He also despises it when a non-white blood cell forms a friendship or relationship with one of his kind. As an immature thymocyte he went through training at Thymus school, where apprentice cells like himself learn to become Mature Thymocytes.
> Now, you can still make an argument that the T cell component of immunity might provide some protection after a previous coronavirus infection. The current study didn’t address this directly
> there are, in fact, people who have both CD4+ and CD8+ T cells that recognize protein antigens from the new coronavirus even though they have never been exposed to SARS, MERS, or the new virus. The paper speculated that this might be due to cross-reactivity with proteins from the “common cold” coronaviruses”, and raised the possibility that there might be a part of the population that has at least some existing protection against the current pandemic.
and
> patients who had caught SARS back in 2003 and recovered ... still have (17 years later!) a robust T-cell response to the original SARS coronavirus’s N protein ..This new work finds that these cross-react with the new SARS CoV-2 N protein as well
There is an open question in the Nature study, about prior, unknown animal coronaviruses which may have previously infected humans and conferred T-cell protection against SARS-CoV-2.
Ah, I stand corrected, thanks! Though not established in the other direction either of course for common cold. But I was wrong to say it was disproven.
> But here’s the key part: “cross-react” does not mean “neutralize” and it does not mean “provide protection from”. These antibodies may or may not have been neutralizing against the other coronaviruses, but they don’t seem to have any such effect on the current one. And in keeping with that, having such cross-reactive antibodies seems to provide no protection against catching SARS-Cov2 or against being hospitalized with it if you do. There’s no difference in the infection/hospitalization rates of the people who had cross-reactive coronavirus serum antibodies ready to go versus those who didn’t. They’re basically useless.
> Now, you can still make an argument that the T cell component of immunity might provide some protection after a previous coronavirus infection. The current study didn’t address this directly, but after these results, it’s at least less likely that that’s happening. The authors make a note of this, and also note that pre-existing mucosal antibodies might exert a protective effect (which this study didn’t examine, either). But prior circulating human coronavirus antibodies, even ones that can bind to the current one – those it looks like we can rule out. Which is too bad.
It's interesting that your comment omitted:
> The current study didn’t address this directly, but after these results, it’s at least less likely that that’s happening.
Perhaps unpopular opinion, but the US vaccination system is about the worst when it comes to preventing spread. Instead, it seems to be attempting to prevent death.
I've always argued that preventing spread would as a byproduct prevent death, but I'm obviously not studied in the field.
Put shortly, I would have vaccinated college kids and working age folks first. They are not likely to die from it, but are far more likely to spread it than elderly and severely diseased folks.
> Perhaps unpopular opinion, but the US vaccination system is about the worst when it comes to preventing spread. Instead, it seems to be attempting to prevent death.
This is by far the most common approach around the world - the same approach is taken in the UK, for example. It's in place for three reasons:
1. We worked out that about 90% of deaths in the first wave would have been prevented if we had been able to vaccinate the most vulnerable groups. This is A Good Thing, both in ite own terms, but also in terms of preventing healthcare systems being overwhelmed.
2. There was no evidence at the beginning that the vaccine prevented transmissibility - only that it prevented serious illness. So the preventing deaths strategy made sense.
3. It's simple to organise and roll-out at speed - and speed is of the essence. Doctors have people's ages and medical vulnerability on record, so you can very quickly draw up lists of who is eligible for vaccination in each cohort. Compare this with trying to arrange vaccination by (say) profession.
I don't understand the relevance of #1, as we have no time machine.
Regarding #2, I think no one seriously thinks the vaccine could fail to prevent spread (it surely is not 100% sterilizing, but everyone acts under the assumption it will vastly reduce spread). "There is no evidence for X" can be said for the vast majority of values of X, since most X are impossible and/or too time consuming to study. This includes, for example, X = "the best way to use the vaccine is to give a first round of second doses before a second round of first doses". But we often have to make decisions in the face of imperfect data.
#3 is ridiculous because the logic appears to be, "the best rollout plan is the one that's easiest to enforce". By this logic, we should line up by height, like we did in elementary school when heading to the toilet.
Preventing deaths and reducing the load on the medical system is absolutely necessary to move forward. If we have vaccinated a good chunk of the elderly and have guaranteed vaccine availability for them, we could open up the economy without fear of the medical system being overloaded. The main reason we shutdown was to prevent the load on hospitals. It has a cascading effect on anyone seeking care.
(Personally know someone who’d have gotten a diagnosis and treatment earlier by at least a couple of months if not for Covid)
Minimizing death at the expense of a slightly longer pandemic doesn't seem like an unreasonable choice in a situation that lacks any perfect solutions.
> the US vaccination system is about the worst when it comes to preventing spread
You have to take a few factors into account when deciding if preventing the spread is your objective. Given the staggering number of cases already out there, the time it takes to vaccinate so many people, and the number of people not willing to be vaccinated, your preferred strategy would be slow (if it worked at all, due to some people refusing to be vaccinated).
In addition, people in the high-risk groups are not fully isolated. Some work, some walk around without masks, some travel. People tend to cluster in age groups, so if one person in the 65+ group gets it, they're going to interact with others in that age group. If a college student gets it, the probability of sustained interaction with someone over 65 is much lower.
That's an argument that can be made with numbers. The problem is we don't really have any. Your assertion that young adults are most likely to spread certainly seems plausible, but the truth is we just don't know. So we made a relatively conservative policy choice and chose to take the low hanging fruit of reducing severe cases at the potential cost of a longer pandemic. It seems reasonable to me, given the facts on the ground.
If you want to pick a nit with US vaccination policy with better grounding, aim at the fact that, with the two-dose mRNA vaccines, we're prioritizing the second dose much more heavily than we should. Numbers after a first dose show something like 70% effectiveness[1]. We should be getting everyone their first dose NOW and not wasting all that effectiveness on the comparatively less impactful booster.
[1] Which is to say, a "1-dose" Pfizer or Moderna vaccine is almost exactly equivalent to the actually-single-dose J&J vaccine.
It will certainly be interesting to follow the studies that will come out on this over the coming years. There are numerous different approaches being taken to vaccination that can be compared. Most of Canada is giving first doses to essentially the entire adult population (which is expected to take a few months) before beginning second doses. Indonesia is focusing on vaccinating young and active people - those most likely to spread the virus - before those most likely to die from it. It will be interesting to see how results compare.
By the way, I've seen that the mRNA vaccines are even more effective than that after the first dose, if you just consider the period from about 10 days onward, ie after it has had a chance to kick in. Here in BC they're quoting a demonstrated efficacy of "up to 90%" from 10 days through to at least 3 months.
Agreed. Before I was vaccinated I read all the numbers I could find. Apparently all 3 show something like 90 percent effectiveness after 3 weeks, even without a second dose for those that ask for it. Seems much more effective to let everyone sit at 90ish, rather than halving the supply for an extra few percent.
Setting aside the topical question of whether it's young adults or younger/older demos that drive the spread, we do have data and modeling to suggest that superspreading events have driven most of the infections [1]. If that's the case, then I think there's a question to be asked about which cohort is more likely than others (if any) to drive super-spreading events.
Well no one -likes- getting covid but there's a far cry from dying from it as the groups who are more apt to want to get it first. If you want to use a more statistics based approach like "well we're going to vaccinate those who are most likely to spread it" (say 20 somethings or republicans who won't wear masks) the general public is not going to go along with that and start making calls to congress critters really quickly since they are afraid memaw is gonna die because she can't get a vaccine while all the college kids throwing ragers on the street are now effectively just a bit safer than before (they were already highly unlikely to die from the disease). Americans by and large do not understand statistics (or even the scientific approach in general) to minimize spreading but "getting shots in arms of those most likely to die" has an undeniable "folksy" logic. The most important thing (the 90% problem) is to get vaccines cranking out as fast as possible and into people, everything else is background noise. I would have been fine with a randomized system based on a voluntary signup list.
It’s not a scientific problem. The scientific solution to contain the pandemic would be a full 21 day absolute shutdown of everything with people surviving on rations. It becomes a political problem if you try to do that in any functioning democracy.
Decisions made about people must have a feedback loop to learn from how people react to it. For example, the lockdown became ineffective when it was extended too long. People were initially very compliant. We were told it’s only till we can prepare our hospitals and prepare a contact tracing strategy. It was convenient for politicians to extend the lockdown than solve those two problems. Net result was that people started ignoring the lockdown more and more. Police can enforce bans on outdoor gatherings; people simply gather at home.
It’s precisely because we ignore the human element that we keep dragging this.
> The scientific solution to contain the pandemic would be a full 21 day absolute shutdown of everything with people surviving on rations.
It is not even a guaranteed solution. It will bring back cases to almost zero. In some rare cases, incubation time can be way longer than 21 days, you are also going to have people with weak immune systems that can contain the infection but not eliminate it completely, plus all the bad things that can happen: mutations, animal transmission, etc...
Then, if we just go back to business as usual after the super-lockdown, it will spread again, just as it started. As long as R>1 there is no way to win. And for now the only way to keep R<1 is to make our lives more or less miserable (today's solution), herd immunity through infections (and let millions die), and herd immunity though vaccines (our goal).
There was no lockdown in any state in the USA. There were instead these totally unenforced “stay at home” orders which people ignored with no consequences. Emergency public health directives during a catastrophe do not need a feedback loop: they need to be enforced, regularly and visibly. That never happened on the USA, and the results have been tragic and predictable.
I agree it's a political problem - a political solution is proven by Asian democracies and Australasian democracies. As you say, it was pretty obvious that a 21-day lockdown with appropriate testing and follow-up would have resolved this issue in any country.
The people's right to have an opinion does not change the truth, that an indefinitely long half-lockdown is a bad compromise between opinions.
Why not? Just because a bunch of people hold that opinion? Political change happens despite groups of people not wanting it - that's almost the definition of politics.
Scientists working for the UK government at Imperial College rejected lockdown as a plan (even what we have now in the UK) because they found it not politically viable: that's a danger to everyone.
> Put shortly, I would have vaccinated college kids and working age folks first. They are not likely to die from it, but are far more likely to spread it than elderly and severely diseased folks.
Many people agree with you. Vaccinating the most mobile people and isolating the most "immobile" (retirees, children, sick) is very logical.
My guess is politicians know it but they would never make such a decision. It'd be a political suicide.
(Also, sorry for the vaguely propagandist source -- I originally heard about this on a podcast and am having trouble determining which, and this doesn't seem to be getting much coverage in English-language print media.)
Countries that have stopped or at least controlled the spread can prioritise vaccinating younger population as that is unlikely to result in more deaths. Singapore has vaccinated its medical personnel (anyone working in a hospital or clinic) then 70 years old and above. Now it is moving to 60 year and above and all the front line workers like teachers, bank tellers, shop attendants, taxi/private drivers etc. They are not facing thousands of deaths so can prioritise protecting the most vulnerable as well as cut off the most likely high spread events.
Fair, but no other country(admittedly) save perhaps Brazil or Italy has had anywhere near the spread of the disease, either. In places the disease isn't rampant, I think the approach makes more sense.
The issue is, something like 80% of the deaths and hospitalizations come from about 20% of the people. It is far quicker to vaccinate 20% of the population than it is to vaccinate the 80% (will less than 80 but more than 20) that covers the group you mentioned.
If course the us didn't do that...
This is a hopeful but possible take. But the 501Y.V2 (B.1.351) and 501Y.V3 (P1) lineages have the mutation within the conserved region for coronaviruses near the spike protein cleavage site. These show massively (1000x) decreased monoclonal antibody binding for original genetic sequence designs. It's better for the mRNA vaccine produced human-body-made antibodies which show only 5-10x reduction in binding.
But antibody binding isn't the full story and there may be T-cell stuff helping too. The data seems to indicate updated spike protein designs will be needed but if there's other stuff going on we don't know about old spike vaccines could still work. I can't say it will definitely help because the vaccine rollout is so slow and air travel is so fast that this negative pressure will probably provoke more variants as long as host numbers remain high.
The monoclonal data is less concerning since the human antibody response is polyclonal. It’s not surprising that this virus can escape from a single targeted antibody and if I were in pharm, this is why I wouldn’t spend billions on a mAb drug. I agree that the decreased convalescent plasma effectiveness is not ideal but I doubt this virus will be able to fully escape the mRNA vaccines on a population level.
Polyclonal antibodies against spike + t-cells + herd immunity should be enough to quell this pandemic. At least I hope so.
"The company commented that compared with other monoclonal antibodies, "VIR-7831 binds to a highly conserved epitope of the spike protein, which may make it more difficult for resistance to develop."
Vir Biotechnology's CEO George Scangos, Ph.D., commented, "These exciting data with a single antibody against a conserved epitope bring us one step closer to delivering an effective new solution to patients around the globe."
I guess I'm just skeptical that anyone can be truly sure of which exposed epitopes are conserved (I haven't seen data on this residue or drug, these are just my thoughts). Given that we're talking about a three dimensional structure, you really need a number of conserved residues in physical proximity to have an inescapable monoclonal antibody. It seems quite possible that there aren't any targets like this and that only a polyclonal immune response, or maybe a cocktail of monoclonals, can be effective in the long-term.
The vaccines create a much more potent antibody response than the titers we see in convalescent plasma. 5-10x less binding probably translates to somewhat reduced efficacy (no one really knows, but 75% vs. 95% might be a reasonable guess). Of course, this is a really complicated thing, because it's not just the immediate antibody response, but also the T-cell response, and also how quickly on a subsequent infection the set of antibodies develops and broadens even more.
We do know that e.g. in Israel where there's very high amounts of vaccine deployed and nasty variants, that case control studies show a large effect still.
I live in the Azores on an island with less than 15k people which was mostly closed last year. There are only two ways to enter the island: the port and the airport there isn't a lot of movement and everyone coming in is tested twice. On top of that people here are terrified of the virus and take it very seriously (masks, distancing, etc) and can even be hostile to newcomers.
Still, cases keep popping up even without systematic testing. There are no deaths or even ICU cases but the virus keeps finding its way in. I believe that, like New Zealand, we are just postponing the inevitable.
I believe that, like New Zealand, we are just postponing the inevitable
New Zealand (and Australia) don't have cases, because every single traveler who enters those island nations is kept in hotel quarantine, and tested multiple times before being released only after the quarantine period ends. It isn't the same as testing people when they come in and letting them straight into the community if they test negative.
That said, with vaccines now being rolled out, it may well be that these countries managed to dodge the bullet. It's hard to see what was "inevitable" about Covid, except the dogma (still promoted by the WHO, when I last checked) that travel bans are bad.
New Zealand and Australia have had cases outside of quarantine despite every single traveller who enters those island nations being kept in hotel quarantine, tested multiple times, and being released only after the quarantine period ends. Some of those cases are directly traceable to quarantined travellers, some aren't. In any case, even those measures which aren't practical except in an island nation aren't effective enough to prevent outbreaks when implemented on a larger scale; the bigger the country the more opportunities for one of those cases to turn into something that's not easily controlled.
Some of those cases are directly traceable to quarantined travellers, some aren't
One of those countries has been able to trace all cases in the last few months and makes extensive use of genomic sequencing. The leaks have all come out of hotel quarantine breaches. I believe that some Australian states that do not receive overseas travelers have not had a single case in months.
It may (or may not) not be feasible for bigger and non-island countries, although I suspect that the border closures will happen far more swiftly if there's another pandemic in our lifetimes.
The state which has the most international arrivals (NSW) just had its first locally transmitted (ie not in hotel quarantine) case in 55 days.
The positive case is a security guard that works at quarantine hotels. Immediate and immense efforts have been put into place to contact trace as many contacts as possible, and to sequence the genome to understand the direct link between existing cases.
We expect these occaisonal breaches in quarantine, and as long as they remain occaisonal they are relatively cheap and easy to contain. Meanwhile restrictions continue to ease and life is almost as normal as you could want - and will certainly be even better once the vaccination program is in full swing.
China successfully followed the same strategy, so the strategy certainly can work for large, non-island countries.
China had a few outbreaks (after Wuhan, obviously), but it responded to each one with quick restrictions on the affected location and mass testing of everyone in the region. That worked to contain these subsequent outbreaks.
As a result, China has been essentially CoVID-19-free for about a year now.
It's hard to tell what on earth is going on in China because a lot of the information coming out of there seems... dubious. As you say, they've had a few outbreaks which they responded to with large-scale lockdowns and mass testing, but if you believe their reporting the mass testing generally didn't find any cases at all which (if accurate) would mean the whole thing was for nothing. This seems unlikely. There were also weird WTF moments like in-hospital spread in a major city in a border region with a known outbreak going undetected for way too long at a time where even western countries that were "failing" at testing had enough in place to detect that. Also, a lot of the information about the source of the outbreaks and their successful methods for eradicating Covid is really obvious propaganda. On the other hand, their hospital system doesn't seem to be collapsing under a mass of Covid cases either.
It's not that difficult to know what's going on in China. There are many millions of Chinese people who call friends and family outside the country regularly. You can go read Chinese social media. There are Westerners in China who post to Western social media. There are even many people on HN who live in China.
> if you believe their reporting the mass testing generally didn't find any cases at all
That's not true. Their mass testing typically picked up further cases, which were isolated:
* In the June 2020 Beijing outbreak, mass testing uncovered over 300 cases.[1]
* In the October 2020 Qingdao outbreak, 9 additional cases (beyond the original three) were caught by mass testing.[2] That suggests that this outbreak was detected early.
* In the October 2020 outbreak in Kashgar, over a hundred additional cases were detected through mass testing.[3]
And of course, there was a more widespread outbreak in December (still concentrated in the Northeast), which peaked at over 100 new cases a day nationwide, and which was stopped with widespread lockdowns and mass testing.
> Also, a lot of the information about the source of the outbreaks and their successful methods for eradicating Covid is really obvious propaganda.
I assume you're talking about the cold chain. I don't see how that's "obvious propaganda." There's good evidence from contact-tracing that some of the subsequent outbreaks originated in people who work in the cold chain. It may seem strange from an American or European point of view, because the cold chain is way less of a problem than the literally millions of infected people walking around in Europe and the US. But in a country with essentially zero community spread and strict quarantine at the border, much less common pathways become a concern. It only takes one person touching a contaminated package and then touching their eyes to set off a new epidemic.
> There's good evidence from contact-tracing that some of the subsequent outbreaks originated in people who work in the cold chain.
Well, that's technically true. It just probably didn't come from the goods being handled like China claimed. In particular, formites and surface contamination of any kind don't seem to be a major source of transmission, and the Beijing outbreak they originally used this to explain seems to actually trace back to infected truckers travelling from somewhere in China with a previously-undetected outbreak that wasn't noticed before because locations outside Beijing didn't have the same level of testing. That is, they found it within their cold chain because that was where they were looking. This is also a lot more consistent with what we know about how Covid is transmitted.
> formites and surface contamination of any kind don't seem to be a major source of transmission
When there are millions of infected people walking around breathing and coughing, then fomite transmission is not a major source of transmission. But it is a source of transmission, and it could become the dominant source of new introductions of the virus into the country if quarantine of travelers is good enough (to go to China, you generally have to get a negative PCR test before your flight, then quarantine for two weeks in a special hotel on arrival, and finally get another negative PCR test). That's not to say that cold chain was actually the source of the Beijing or the Qingdao outbreaks, but there's evidence that points in that direction. In other words, this isn't simply propaganda.
But the larger issue that we were originally discussing is the overall situation in China. There clearly has not been significant community transmission over the past year, showing that the strategy (sharp lockdowns followed by strict border quarantines and mass testing during localized outbreaks) has been effective.
This is enforceable in remote island countries, but in ie Europe its not. You can't 100% lock the borders, there would be shortages of basically everything, from food to materials used in all industries. Europe is not so unified as US for example, there is a lot of independence, for better or worse. Food is transported on trucks, till it reaches from Spain say Poland it crosses minimum of 4-5 countries, each with their own covid situation, laws, rules, bans etc.
If we knew back a year ago how bad things would get and are still getting, I believe such a lockdown for say a month could pass, otherwise not and there isn't a central authority that could enforce it. And saying it was to be expected doesn't make much sense, spread of predicted outcomes was basically between yet another flu to another spanish flu.
What could've ended the pandemic around 6 months ago was human challenge trials on vaccines, and paying much more for earlier supplies of vaccines including those donated to other countries. (What counts as an impossible supply challenge is very different at the $500 price point than at the $50 price point.)
> What counts as an impossible supply challenge is very different at the $500 price point than at the $50 price point.
Considering the insane profits pharmaceutical companies are currently recording, the issue has more to do with these companies favoring their benefits to the detriment of the general population which should come as no surprise to anyone having experience dealing with a pharma company.
The issue is particularly prevalent in Europe because as usual, apart from some grand posturing in the media, Europe will do nothing to fight back.
I think most of the companies are selling the vaccine quite cheaply.
Moderna and Pfizer are asking for 15-20 $ / person for vaccine that has value of thousands of euros.
Which, as Eliezer notes, is part of the problem. That together with flexible delivery schedules in agreements mean that companies have little extra resources and incentives to invest in fast vaccine production.
Comparing an island nation of 5 million people, that can effectively close it's borders and "avoid" new focuses of infection, to countries of 100+ million of people, where the difficulties of border closing are effectively unsurmountable, is extremely disingenuous. The whole approach governments took in facing this pandemic needs to be studied in the next decades. It's an eye opening thing to see how viruses spread pretty much the way they do, and there is almost nothing we can do to stop it. It's really humbling to see that if you keep everything open (i.e. Florida) you get the same results as if you make your population effectively stop to live for one year (i.e. California).
well vietnam also did extremely well. and new zealands managed isolation (which i just went through) could easily be replicated anywhere there are hotels
In my country of 8 millions (Switzerland), about 340'000 people commute to Switzerland each day to work [1]. These people come from Italy, France, Germany and a bit from Austria. A lot of these people do important work, such as working in hospitals, administration, services, ...
Locking down the borders completely would just have been impossible. You would be suddendly in need of nurses and doctors. Sometimes, more than 50% of the personal in bordering hospitals are cross-border commuters [2]. Yes, you could discuss on how Switzerland is taking advantage of "cheap" labor from neighboring countries, but it does not change the fact that for Switzerland, closing completely the borders (with 14 days isolation) is just an impossible task.
Thailand’s 50m people with 3,000km of mostly unpoliced border, they made it work. Vietnam made it work. Locking borders early and moving to quarantined entry apparently works, and when some knobs walk over the border with Covid, as has happened with both countries, you can unleash an almighty track-and-trace and isolated lockdowns because the health system isn’t already on its knees.
They're not islands in a strict geographical sense, but there are a dozen or so countries which are de-facto islands for any practical purposes - accessible only through large bodies of water, with land borders mostly impassable or crossed so infrequently that they don't matter.
South Korea, North Korea, Finland, Vietnam, several central American countries and others. Even China fits the bill. Not sure how frequent traffic across Thai borders are, but my impression is that SE Asian countries are not very well integrated.
Track and trace works way better when you have 20 or so people infected than when you have 100,000. It's not even the health system, just the logistics of tracking everyone down. I kind of experienced both - the first in Koh Lanta and the second in London.
Its likely illegal for California to close its borders to Florida. But that probably would have slowed the spread significantly, at least in the 3rd wave where the Mid-Western / anti-mask states led the 3rd wave.
This country was in this together. For better or for worse. Closing the borders of states was never an option.
> Its likely illegal for California to close its borders to Florida.
I wonder if that's really the case. A year ago I'd say the same for Australia. Yet most Australian states closed their borders at some point as a response to local cases spiking. (I agree it's less practical in the US, but I do wonder about the legality)
Whatever the answer I feel like it would take the courts a few weeks at least to figure it out. California (or more realistically Hawaii) could have had a full three week border closure before anyone settled the case law.
Not very many roads enter California, as it has natural geological borders. An ocean to the west, hilly forest to the north. On the east, a 3 km high mountain range which leads into a hot desert, cut by the mighty Colorado. The terrain is a lot more forgiving to the south, but there’s an artificial border with Baja California there.
Plus, most of the infrastructure is there for the agricultural inspection stations. Just use it to stop human disease instead of plant disease.
And if I kind of zoom into Google maps I count 36 crossing between the Oregon/California border just between the Pacific ocean and I-5. Sure, a lot of those are probably logging roads and such, but that's just a 60 mile stretch.
I do not live in the US, but I love that your system allows you guys to have effectively 51 experiments on how to deal with the spread of a virus, and see the results of every strategy. Do you really think that, if you can't even control your borders between states, your border on the south with Mexico for instance, would ever be effectively controlled to avoid the virus to come through it? The complete failure of California (even when compared to states where the demographics tend more to the older generations) tells me everything that is needed to understand if the lockdown approach works or not.
California is far from a monolith, though. Alameda County, where I live, hasn't been that bad, and has had a strong lockdown policy. Other parts of california have larger populations of anti-maskers. And the California prison system has been a complete disaster, largely because of incompetence and inhumanity in the administration.
It's a distant island nation at the end of the transport network.
One of the reasons New York, London and Brussels have been hit so hard is that they are global hubs in the world transport and financial power networks.
Not really. There are two basically insurmountable problems with taking New Zealand's success and expanding it to the entire globe. Firstly, the effectiveness of this is limited by wherever it works the least well. Secondly, even if everywhere could implement the same measures as New Zealand as well as they did, over that large a scale there would be places which had much worse success just through random chance alone. You can see a few places where New Zealand got lucky already, like the recent outbreak of unknown origin not spreading as widely as it might've or the infections amongst border workers back when they weren't being widely tested. You can also see this in Australia, which is similar geographically but bigger and has taken many similar measures with slightly worse results. Scale up three orders of magnitude, and I've no doubt fun new failure modes will appear which aren't even visible yet.
China is the most populous country on Earth, and geographically, one of the largest. It has followed a similar strategy as New Zealand and Australia. That strategy has worked to keep the country essentially CoVID-19-free over the past year.
It's what I've been told by numerous people who live in China. It's what I see on Chinese social media, and it's what Westerners who live in China are saying on Western social media. I'm sure there are many on HN who live in China - they can also tell you what things are like there.
If there were a major ongoing epidemic in China, it would be impossible to hide. Hospitals would be under the same sort of pressure that they are in Europe and the US. People would have family members and friends who got sick or who died. That's not happening. China is simply too tightly connected to the rest of the world to keep things like this a secret. In December 2019, the existence of the outbreak in Wuhan was known around the world within days of the first patient test results coming back.
Even Western media began grudgingly admitting several months ago the virus was essentially gone from China. For example, German/French public radio did a pretty interesting documentary on post-CoVID-19 Wuhan. The first scene is in a packed discotheque:
>It's what I've been told by numerous people who live in China. It's what I see on Chinese social media, and it's what Westerners who live in China are saying on Western social media.
Yep, that's how censorship works.
I'm sure you won't see too many people talking about Tiananmen Square on Chinese social media either, but that doesn't mean it didn't happen.
Are we really going to pretend that the Chinese government hasn't been heavily censoring information which makes them look bad?
Early on in the pandemic, the Chinese covid death counts started to skyrocket, and activists within the country were using Github to make sure this information did not get 404'd. The same day these activists were dissapeared, the skyrocketing "official" chinese covid death count immediately went down to "0", where it has remained ever since. When using Google to browse the death counts by country, you can't even look at the death counts for China, the button is disabled.
China doesn't have the power to censor Western expats on Twitter, or the millions of live conversations going on at any given moment between people inside China and people outside. This view of China, that it's a black box that information can't escape out of, is simply not reality.
>China doesn't have the power to censor Western expats on Twitter,
Yes, they do, directly and indirectly.
Directly: Li-Meng Yan, the Chinese virologist who blew the whistle on covid in December 2019, but the Chinese government covered that up. She defected to the US, and published a research paper critical of the Chinese government, and Twitter banned her account.
Indirectly: How likely do you think it would be for the chinese government to renew an expats visa if they were doing activist work like the chinese activists who got dissapeared for reporting covid deaths on Github? They didn't even let a WHO investigation team into their country for almost a year
Li-Meng Yan didn't blow the whistle in December 2019. She's a Hong Konger who started making crazy claims months after the outbreak began. She flew to the US, claimed she was persecuted, and now works for Steve Bannon. She's made all sorts of crazy claims, including that SARS-CoV-2 is a bioweapon.
The first pneumonia patients in Wuhan got their test results showing a suspected SARS-related coronavirus on 27 December 2019. The local authorities put out an alert on 30 December, which was instantly noticed by people around the world who track emerging infectious diseases. In other words, health professionals around the world knew about the Wuhan outbreak within 3 days of the first suspicious test results.
I don't think you realize the sheer volume of communication between people in China and the outside world. Many millions of everyday people are in regular contact across the border. There are many millions more people with VPNs who say whatever they want on Western social media. Even Chinese social media is way too active for the government to thoroughly monitor. Almost anything major that happens in China nowadays is known about outside China pretty much instantly. The idea that there's been a massive epidemic underway in China over the past year and that the government has been able to keep that information from leaking to the outside world is utterly implausible.
> They didn't even let a WHO investigation team into their country for almost a year
Which WHO investigation? The WHO visited on 20 January 2020, just three weeks after the outbreak was identified.[1] Months later, for political reasons, the Australian PM started demanding an "investigation." China didn't like the accusatory nature of the Australian demands, and it took months to negotiate a process that all sides considered reasonable. But the WHO was in Wuhan long before Australia began demanding a different sort of investigation.
As far as I know, it was well-reported in the papers that the WHO team was first blocked from entering. And then once they were allowed in, all the data was sanitised for them.
First of all, I'm talking about the WHO team that went to Wuhan in January 2020, not the team that went there a year later. The WHO was on the ground in Wuhan within weeks of the initial detection of the outbreak.
Second of all, you should take the claims of Western media about China with more than a grain of salt. The WHO team that went a year later wasn't blocked from entering. A few team members began traveling to China before their visas were approved. The data wasn't "sanitized." One team member said he wanted to see additional data. The newspapers trumpeted that, claiming that China had hidden everything. Other members of the WHO team then criticized the newspapers, saying that they had been given extensive access to the data they wanted.
I’m skeptical. Even countries like Singapore have constantly had 1 or 2 locally transmitted cases per month they can’t trace.
Now multiply that across 170 countries some too poor to do what Singapore did.
If every country had locked down like NZ, we would have just had a series of lockdowns and flare ups and more lockdowns. It certainly would have kept the case numbers much lower but can you imagine the fatigue after going through your 12th lockdown?
I can imagine the fatigue of what I’m currently going through of constantly locking down for 4 months at a time!
Compared to that, having to lock down every couple of months for a week or two doesn’t seem anywhere near as bad. Oh, and we wouldn’t have 130,000 dead in the UK and 500,000+ dead in the USA!
A couple of weeks is basically the bare minimum. New Zealand seem to have gotten a little lucky with their latest outbreak; one or two people not noticing their symptoms, or going for a walk with someone different, or interacting for a little longer at a restaurant and they could easily have ended up having to lock down for months like Guernsey or the Isle of Man. (Arguably, it's still a little too soon to be sure they've gotten away with it.)
So the population of a whole city is normalized on lock down as if they were inmates of some large prison camp, while the government uses all sorts of surveillance mechanisms to track whoever they please freely for some very marginal public health benefit, and this whole situation is considered "great". What kinds of things have been normalized in the supposedly free countries by this pandemic.
You assume wrong about my nationality. One doesn't have to be Trump-loving caricature of an American to deeply mistrust restrictions of basic individual liberties.. And if not marginal health benefit then most definitely highly ambiguous, debatable health benefits as far as a large weight of evidence is concerned. Some countries with lockdown measures have had lower mortality rates while others with just as strict rates have had high mortality rates, and many countries without much in the way of restrictions have had mortality rates little or not at all different from those of other countries with severe restrictions. There is no existing consensus here and all evidence seems to be all over the place. The themes I mentioned in my previous comment however are normalizations that bode dangerously for the future of supposedly free countries, the future of social globalization (a good thing overall because it strongly counteracts nationalist tendencies) and none of this is to even mention the still unknown long term consequences of the vast economic destruction cause by so much callous but ambiguously backed lockdown policy in so many places.
To put your numbers in perspective, in a population of 330mio with life expectancy 70-75y (USA numbers), every year around 4mio people die for some reason or another. Not saying covid is not a problem, but these numbers don't really support the claim.
Yeah but that's unrealistic proposal that looks nice on paper, but completely ignores real human nature and how complex and diverse real world is.
Who has the authority for global shutdowns? Nobody. Many nations wouldn't agree on that and political discussions would be endless, everybody has their own agenda regardless of virus. Can you imagine some Europeans telling USA 'OK now whole of your nation will stay at home for 2 weeks'. Not going to fly on any US level. Or Americans to Chinese.
Globally it haven't been handled OK by any means, but these naive suggestions don't help getting a workable solution.
'If only all people behaved rationally' can be wished in any discussion, sure, but it doesn't get us anywhere closer to solutions.
Well, no, that’s exactly what I’m saying would not be the case. The longer lockdown would not need to be anywhere near as strict as the lockdown that comes after a month of opening everything back up.
Wow, so now instead of the ‘three weeks strict lockdown to stop the spread’ fantasy we now have this ‘lockdown light’ idea. Where did this theory come from?
The only chance for lockdowns was in China, early on. Being a country with virtually unlimited money, manpower and an authoritarian regime Covid could have died in there. Quarantine enforced by millions of soldiers and police.
Once out, you're dealing with about 200 countries divided in tens of thousands of localities and hundreds of thousands of politicians with their own goals and beliefs. So, not doable.
That's impossible. China is not North Korea. All it takes is just 1 asymptomatic infected person to leave the country - perhaps 1 hour before the hypothetical country-wide lockdown - for the virus to spread.
No, it's even worse than that. Signs of covid have been found in Europe dating back to October 2019, before anyone in China knew that this existed.
Besides, western countries didn't take the virus seriously in the beginning at all. Even a month after the Wuhan lockdown, the Dutch didn't take much action, while Trump said it's just the cold. The attitude was basically: it's only a disaster in China, outside China it's not serious.
> The attitude was basically: it's only a disaster in China, outside China it's not serious.
Your comment is on point. I'm certain that many European countries benefitted from the escalation in Italy and pictures of army trucks filled with body bags. From then on, most took the virus a lot more serious.
'It's only a disaster in X, in our country it's not serious' has been a recurring theme and it's one of the things that makes me bearish going forward.
It has been already analyzed in very fine detail, what you mention is an obvious double/triple check. If you have a sample that changes whole global narrative, you can make enough detailed tests on it to have statistical chance of error close to 0. Too bad they don't have earlier samples, we could possibly find it way earlier.
It wasn't October 2019, actually Italy had September 2019! A few countries had it back-identified before official Wuhan ones. France had December. Its very well possible that Covid originated elsewhere, but that's another topic.
I remember the Chinese guy Zhong Nanshan saying if the world took his/Chinese advice, basically Wuhan like policies, that the whole thing could be gone by June 2020. But I guess with Trumps and Bolsonaros running countries that wasn't on the cards.
i'm very surprised to see remdesivir mentionned in this article at all... Isn't this drug officialy not working at all against covid-19 , and as such should be banned because of perfusion side-effects ? (in addition to the fact that it seems to be known to increase the amount of virus genetic mutations in people treated with it)
Here in the Czech Republic, doctors in Brno are trying a combination of remdesivir and convalescent plasma in oncological Covid patients. They say that the combo has, so far, worked much better than either of the components in isolation. Out of the small cohort, they lost no one so far.
That's the treatment that I got back in September in the US. I think they stopped using Remdesivir since then because it didn't correlate with any positive outcome. It also was destroying my liver, so they had to cut off the treatment halfway through.
Maybe the total balance of results is better for immunosuppressed oncologic patients.
Or maybe it is just a form of medical nationalism, given that the leader of the Remdesivir scientific team, Tomáš Cihlář, is a Czech scientist.
We had some critical patients improve and heal on remdesivir, though. I wonder how big of a role genetic diversity plays. There are many uncertain suspicions that Covid hits some people harder than others based not just on lifestyle, but things such as blood groups.
Research into that will be a good PhD material for years to come.
One thing I've learnt from the whole C19 treatment debacle is to never ever trust any single study.
Unlike computer science where if you test something and it works once you and then you expect it to work for everyone, in medical research if you see an effect in one treatment study you probably won't see the same effect elsewhere.
For treatments (unlike controlled vaccine studies) the cohorts are too small and there are too many other variables.
Journalistic interpretation of these tiny, rushed studies has also been god awful since the beginning. This is true during the best of times, but every clickbait headlines spreading disinformation during an actual pandemic should not be tolerated, especially amongst the more reputable news sources (looking at you NYT).
This right here. If people look at the actual study, they'll see the number of caveats and various exact conditions where the study proved something, whereas the media tends to pretend that those caveats or conditions don't exist therefore, the study works everywhere. That's why people don't trust science, "oh, its probably wrong again".
Some of the worst offenders have been scientists, who promote their own studies (eg, the French hydroxychloroquine studies).
It's possible to pick holes in these studies if you know the field. But these holes aren't pointed out in the papers themselves, and peer review doesn't stop this.
Peer reviewers are experts in the field. So they know if they are looking at a 30 person study it isn't conclusive, and wouldn't expect the author to state that. It's just assumed the readers know that.
We see the real impact of this with things like the Vitamin D studies. Experts know that Vitamin D deficiency is highly correlated with age and other health issues, but that the causation chain is "Person is unhealthy so doesn't get outside as much so gets less Vitamin D, and in some cases are deficient which can make health issues worse". Non-experts read the report and see the causation going the other way, ie, they think: "High Vitamin D fixes health issues".
I broadly agree but I usually trust one of the big ones (e.g. ‘recovery’ in the UK) since they have pretty big sample sizes and seem to be on top of stats.
Even in computer science I don't think that holds. Lord knows there are enough stories about issues with unusual hardware and unreproducible heisen-bugs that I would never assume that something will work for everybody just because it worked once, on your own machine.
From what I understand Remdesivir doesn't show results in mortality, but has positive results in recovery speed of patients who otherwise would not have died. I believe it shaves about 5 days off the supplemental O2/ICU phase, which decreases the window in which you can develop other complications and also gets your butt out to free up hospital resources quicker.
Mexico just issued an emergency use authorization yesterday. Japan, Canada, and the EU have also authorized the drug for COVID patients.
I’m as skeptical of your last parenthetical as you should be about remdesivir’s overall effectiveness. In any case, the effects are too small to matter.
No, my thirty-five-year old sister-in-law was given remdesivir twice during her stay in a Los Angeles hospital during the December wave, and while she had early stage covid pneumonia she was not in the ICU.
I also hope we will continue to be more careful about germ control from here on out in myriad ways. I hope we do not blithely go back to "business as usual" in a way that fosters future pandemics as if we learned absolutely nothing here.
I worry also about an overreaction. At some level people who can survive a virus with little to no symptoms are better off contracting it than not, if only to form the antibodies to be ready for future mutants they might come in contact with. The behavior changes we make because of COVID could be dooming a lot of people to one day encounter much worse mutant viruses they could have been ready for.
I really hate this kind of logic. I get where it comes from but I still hate it.
I have a genetic disorder that causes a compromised immune system, so germ control is my life. My life got better in some important ways with the entire rest of the world being less germy and disgusting.
About one of out every five people is officially labeled "handicapped" and at least one study suggests that up to three out of every five people may have more minor impairments that they mostly cover up and don't want to label as a "handicap" because it's stigmatizing. A great many people with various handicaps are immunocompromised or otherwise vulnerable.
A lot of handicapped people saw some things improve for themselves while the entire world temporarily felt that germ control was super important. As one of those people, I am very concerned that "business as usual" will be a terrible thing for me.
I've tried to figure out how to write about what kinds of best practices I would like to see, but that never really gelled in part because I became very concerned it would make me a target for the fear and anger of a lot of people during a global crisis. I didn't want some sort of lynch mob to descend upon me while much of the world applauded their depravity because, hey, scapegoats rather than solutions seems to be a very popular pursuit in the world generally, even during "normal" times and folks seem to double down on that during crises.
Maybe I will still find a way to write about it and have some kind of influence on moving the needle gently but firmly in the right direction. And maybe not. I don't have much of an audience and like Rodney Dangerfield "I get no respect" and yadda.
I do not have those problems. I am sorry you do. Sucks.
But, I am definitely not returning to "normal" pre Covid behavior.
I got Covid early on. It was extremely rough. Should probably have been in the hospital, but frankly worried about that a lot given what was happening.
Made it through, as did my family.
Those experiences were why we played it very safe. Lots of negatives in doing that, but there were some positives, damn good takeaways:
We basically saw a no flu season. Haven't caught much more than a sneeze. That is awful nice.
Travel, work, life balance got reset. Turns out a whole lot more can be done without doing those things as much. Good for the planet, good for a lot of people, me, mine.
Health care in the US is broken, and so is our governance. This whole thing has made me see just how severe cost and risk exposure for way too many people really is!
Our response, information distribution, and I could go on for a long while here is frankly and completely unacceptable.
There is real work to do and we have been running balls out and basically ignoring it, marginalizing costs and risks and in general just do not have our national priorities in order.
Just know others hear you. We felt it too. Felt it differently, but I do not think that matters.
> Health care in the US is broken, and so is our governance. This whole thing has made me see just how severe cost and risk exposure for way too many people really is!
There are a lot of people who benefit from health care being broken so I’m very pessimistic if we will see single payer in our lifetime. We all need to keep fighting for it but to be realistic it might not happen in the next thirty years.
There is an order, if not two more who do not benefit, and it is unnecessary.
I agree with you. However, I will also no longer be quiet about it. My own costs and risks have been insane. Future impacted in the negative multiple times now.
Would not have been most other parts of the world.
Frankly, the cost and risk exposure will hit a point where people move in mass, or it won't and we trundle along for a decade or two.
Nobody knows.
What I do know is I have reached a point where I will act in solidarity with others on this matter and will make very aggressive trade offs too. It is now a priority.
I am a dual US|EU (Croatian) citizen, who naturalized (by descent, via my 4 Croatian great-grandparents, even though I only needed 1) as Croatian over the US healthcare system. Because I am an European Union citizen, I can live/work/retire in the EU and EFTA countries (minus Lichtenstein--has an immigration quota), due to Freedom of Movement rights. I have 2 rare immune-mediated neurological diseases affecting my peripheral nervous system, plus type 1 diabetes (autoimmune and insulin-dependent). Anyways, even though the neurological diseases are in pharmaceutical remission, I require a lot of unusual and expensive treatments to stay alive. I am an electrical engineering graduate student, who has studied healthcare systems and delivery, and I understand the logistics and the bureaucracy involved. I am also an expert on processes involving acquiring citizenship. Feel free to shoot me an email, if you want (see my profile).
Ironically, the best resource for navigating the various intricacies of various countries' health systems, globally, with respect to living a long life, is the IMHE group. You know, the group that was famous for the coronavirus projections at the beginning of the pandemic in the USA. All of their peer-reviewed publications are open access, too.
This is probably the most important research article to consult and study (although there are several others): Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories using data from the Global Burden of Disease Study 2016: http://www.healthdata.org/research-article/forecasting-life-...
M4A is socialism and is just too easy a target in the U.S. At some point there will beer a republicans president, and due to the structural advantages it’s likely he will have full control over all branches. Not sure that a real democracy can survive that.
But, I am definitely not returning to "normal" pre Covid behavior.
What would this look like, in practice? Of course on a macro scale we'll see changes like increasing adoption and acceptance of remote work/meetings, but in terms of individual behavior what can or should change?
I assume 10 years from now (barring another pandemic) we won't all be wearing masks and gloves all the time or strictly maintaining a six-foot distance from all other people, but offhand I see myself maintaining a few habits to varying degrees of strictness:
* Consistently washing my hands after touching mail or packages
* Letting packages sit by the front door for a day or two before bringing them further inside and opening them
* Pressing crosswalk buttons with my elbow
* Flushing non-automatic public toilets/urinals with my foot and opening/closing restroom doors with my foot, my elbow, or my hand and a paper towel
* Immediately showering and changing after being in public
* Wiping down groceries before putting them away
* If I need to go out in public while sick for whatever reason, wearing an N95/equivalent mask (not that I had a habit of going out while sick to begin with / I can't specifically recall having ever done so, but if I had ever needed to it certainly wouldn't have occurred to me or struck me as socially acceptable to put on a mask)
* When I return to the gym, consistently wearing gloves (I bought a bunch of full-fingered workout gloves and did this for a week or two last year just before everything shut down, and resumed the habit at home after a sliver of metal broke off of one of my dumbbell handles and got stuck in my finger)
* Maybe continuing to wear gloves while in public in general, or even just semi-regularly using hand sanitizer
Your list is a lot like mine. Giving the basics a higher priority for the longer term, and teaching these to young ones, along with appropriate norms are how I intend on playing it all going forward.
But your genetic disorder shouldn’t be extended to negatively impact others, knowing your unique situation means you need to manage your risks. It’s entirely unfair and a violation of privacy for people to have to be brought into your health decisions and vice versa. Why would it ever be reasonable to expect the government to keep tabs on random strangers just because I have a genetic health condition?
I would much rather die than force someone else to suddenly be required to base their free agency around what happens to work best for me, especially because I am 100% going to die no matter what.
It just seems totally illogical to remove freedoms at scale to prevent something that is ultimately inevitable.
Basically seems like throwing the baby out with the bath water, what’s the point of having a society at all if people have to be micro-managed to the point of being enslaved to each other’s mortality? It just seems so obviously a mistake and a huge slippery slope.
What’s next, they tell us which people have to die so the rest of us don’t have to be burdened with them? That is essentially exactly what this type of government/healthcare overreach is doing.
I shouldn't have to tell people I have a genetic disorder to have them respect my desire to keep their damn hands off of me.
Expecting random strangers to not touch me is not some huge invasive expectation. Quite the contrary: The people who think they are entitled to touch me are being invasive and making an imposition. People should not feel that because I'm poor or an attractive woman or whatever that touching me is appropriate behavior when we are total strangers.
That's just one example and I don't intend to discuss this further with you.
I very much agree to getting rid of the mandatory handshaking habit. And quite some similar customs. Like in the supermarket yesterday, with everyone wearing masks, limited people inside etc. - but then at the cashier I was expected to use the same dirty digital pen to sign the payment by card, like everybody else did. Such idiocity.
But for the rest, do you expect people to continiue to wear masks after this?
In general, are you aware, that the youth of this planet is pretty much on standby since a year? They are not really threatened by covid, yet they have to pay the highest toll in the restrictions - because their life is not established, they have to move around to set up their life. Which they cannot really do now. They could also say, fuck the old and weak, we won't sacrifice more for them - we got to live our lives now - but they are largely not doing it. So maybe it is not such a shitty egoistic world after all?
But for the rest, do you expect people to continiue to wear masks after this?
No, I don't expect people to wear masks as the new norm.
I haven't managed to write in earnest because I think people treat masks like plus two magic items in the game of Pandemic and I mostly hate them and this is not exactly a good place from which to gain an audience and yadda under current circumstances.
Oh, that is surprising, I mean, I hate the masks, too, but my immune system is quite good, so I wear it only for the sake of other people. May I ask, why you object to masks for yourself?
It is an "US" problem. Frankly, we have a number of US problems brewing and we have them due to not having our priorities in order as a people, human beings.
Another way of looking at it is that most people are incompetent at being selfish.
A competently selfish person would realize that having compassion for their fellow human beings is one of the most selfish traits they could ever have.
Indeed. The advantages add right up quickly. In my view, that it does not all end up in a spreadsheet or bank account makes this a harder discussion than it needs to be.
I understand you hold that opinion. Also understand it is a minority opinion. And hey, I get it. Many people do not like to be told what they have to do.
Humans, this place we inhabit works the way it works. There will be tradeoffs.
Managing public health is one of them. There are many others.
Sincerely, I wish you had the option to live in a personal vacuum, "you do you" style, but that option is currently unavailable.
There are some options given you are willing to either forego many of the benefits that come with a well developed society, or accumulate wealth sufficient to isolate yourself.
Barring those, yeah. You are just another member of the public.
Don't get me wrong I'm very open to a cleaner world. I watch videos of people walking around Tokyo and I marvel at the clean streets. Minimizing places for viruses to grow and mutate is a common ground I think nobody would attack anyone for suggesting, if they're well thought out and not attached to something already political anyway.
I totally agree with this. I’m not disabled but I do have a pretty crappy upper respiratory system, and I used to get URT infections regularly, like 7-8 times a year. In 2020? Not one. I think my increased awareness about hygiene and the same from the general public really had an effect. And yes, masks too. If there’s one thing positive I hope we can take from this, it is normalizing mask-wearing when you are sick or expect to be around sick people. I plan to continue the practice myself, and pay much more attention to hygiene and personal space, like not touching people unnecessarily.
Imo it's hard. Different people get different consequences from different approaches. Now, I'm no expert, but I know a little bit about allergies - and I believe it's fairly well known that not being exposed to dirty environments, animals and nature have caused a huge increase in allergies all around the world (but very much the most in the developed world). I guess what I'm saying is that it's not that simple, and a lot comes down to politics.
I believe it's fairly well known that not being exposed to dirty environments, animals and nature have caused a huge increase in allergies all around the world (but very much the most in the developed world).
I keep hearing that but I don't really know where that idea comes from. I am skeptical of that idea.
I don't think things are simple at all. That's part of why my desire to write on the topic hasn't really gone anywhere.
I haven't had so much as a cold in the last... checks calendar... year. Humans are much more capable of containing basic every-day pathogens than we seem to have thought.
Can you explain what you mean by germ control? Covid is primarily transmitted by sustained exposure to aerosols. Much of the disinfecting we are now doing now is essentially performative.
Much of the disinfecting we are now doing now is essentially performative.
Yes, a lot of the things we are doing are performative. Most people don't really know how to use masks effectively and a lot of how people interact with their masks makes things worse, not better.
I work really hard to just avoid being exposed to germs because of my situation. I try to not touch a lot of stuff in public and this is not the norm.
I hate it when people "helpfully" want to get me a cart. I can get it myself. Keep your hands off my cart.
I saw someone blow their nose under their mask just a few feet from me. I wish we would focus much more on messages like "Don't blow your nose in crowded public spaces" than on "Wear your mask." There have been so many incidents like that and I have been toying with the idea of starting an "incident report" file to talk about specific incidents and why this stuff makes me crazy.
I don't like people talking at me unnecessarily.
I don't like people laughing near me. That's almost as bad as people coughing at me.
I will shower as promptly as I can if someone does cough in my general direction or similar.
There's a whole lot of stuff I do to simply avoid germs without having to rely a lot on chemical disinfectants because I'm also chemically sensitive. And I am a lot healthier than I am supposed to be so I know this stuff works.
If anyone has ideas on how I can effectively start writing about this, I'm all ears. I don't know how to get, say, beta readers or some kind of early feedback. I know it's a touchy topic and feedback and some kind of traction would be enormously helpful in trying to write more about this. I can't seem to get that part, so it ends up being very incomplete, one-off comments on the internet, like this one.
Why wouldn’t we go back to normal? We’ve done that after stock market crashes, housing crashes and other pandemics. That’s what humans do. It takes about a decade or two before people assume it will never happen again.
For one shining moment, while the world burned, my life sort of worked because people were willing to let me take a wide berth around them without them glaring at me like I was some evil, hateful bitch for not wanting to be coughed on.
I don't want the pandemic to persist, but I desperately hope that the end of the pandemic doesn't have such a negative impact on my life as an individual with a compromised immune system as to make me wish it would come back.
I don't think that's an unreasonable thing to hope for, though I'm aware I may well not get it. I long ago got the memo that it's a shitty world full of shitty people and, no, this shitty world doesn't give a damn at all about my welfare or what I want. The world has been not at all shy about letting me know that.
What we learned should be not to decimate small businesses like tossing leaves to the wind “don’t worry we’ll build back better!” and let people decide their own risk taking.
I think that it’s almost more terrifying than the thing itself that more people aren’t mostly incredibly disturbed by the insane violations of privacy and speech.
Literally you should not, in a free society, be able take such injurious actions based on something that the average person cannot even verify.
It should never be that a tiny group of experts just have to be trusted to make decisions for everyone while the vast majority of the people are completely incapable of actually even seeing the threat.
The vaccine thing too is absurd, amazing how quickly a public health crisis becomes an attempt at side stepping private health decisions.
No amount of “but people could die” can justify this, that’s an irrelevant point, because there never a time when it was proper to remove autonomy for such a reason! It’s a total invasion of privacy that the government should even know where most people are at most times, what they are wearing or eating, or that private individuals should be corralled like cattle for the sake of “all cattle”, I just wish people could see what a huge privacy violation it is when a government decides that the most important thing above all else is to try and keep everyone alive as long as possible at the expense of each other and at the expense of freedom to avoid such an arrangement, privacy for bringing you into it in the first place, and opportunity cost of when you end up with no choice due to violent demands of state.
There's a massive difference between contagious diseases with exponential growth potential and the other freedoms you talk about.
For a closer analogy than "what people are wearing or eating", what about "what people drive and how fast in public areas".
The government introduced speed limits, regulations on vehicles, and driver licenses, all of which significantly limit who can drive what, and how fast. All of this is enforced by police.
Why is it fair for the government to do that? Because dangerous driving kills other people too, not just you. It's not a personal choice in a vacuum to drive drunk at 100mph, but a personal choice that kills others.
Covid is similar. Limits on gatherings, requirements to wear masks, etc are all because personal decisions also affect others at a larger scale. A pandemic, when it's not controlled, will spread exponentially and cause significant death and health problems.
I think there might be a reasonable discussion to be had about the role of the government in this, but that reasonable discussion does not start with claims that the government is treating us like cattle or that "but people could die" is not a valid justification for government action.
The chance of people dying is a valid justification. I think it was a valid justification for requiring a driver license, for making drunk driving illegal, and I think it's probably a valid justification for the current restrictions and regulations. You can apply this similarly to some of your other points: a tiny group of experts determine what standards make cars street-legal in the US and decide that drunk driving is dangerous, and their decisions impact everyone, etc.
SARS-CoV2 is not capable of exponential growth. There is nearly one hundred years of epidemiology that shows lockdowns are not effective at containing the spread of highly contagious pathogens. Masks, hand washing, and distancing do help. Having authority does not excuse having a weak grasp of the science.
It's proven that speed limits save lives by 100% of scientists.
There's absolutely no proof that quarantine or any of these Covid restrictions was effective.
There's a study that masks might prevent spread by around 2%. That doesn't seem enough to enforce massive restrictions to me. Sweden and had less deaths per capita then most of Europe and they had minimal restrictions.
Also the scale of the restrictions is different than speed limits.
Quarantine and business shutdowns are massive changes to society and repressive restrictions on financial survival and affect just about every aspect of our lives versus just some targeted change like a speed limit.
What if a vaccine had never been developed?
Would you be okay enforcing these restrictions forever?
There's also no randomized trial proving that parachutes prevent death during skydiving.
But it stands to reason that not slamming into the ground at terminal velocity is good for your health, and it stands to reason that preventing the spread of a deadly disease saves lives.
Countries that have prevented the spread of the disease (China, Vietnam, Thailand, Australia, New Zealand, and others) have orders of magnitude fewer deaths, as a proportion of their population.
The germ theory of disease is also well established.
For SARS-CoV-2, while there are still some uncertainties about precisely how important different modes of transmission are, it's clear that it's a respiratory disease. Quarantine works to stop transmission. Lockdowns like the one in Wuhan or those in Australia work, because they stop infected people from coming into close proximity with susceptible people. This much is understood, despite whatever other uncertainties there are.
The fact that quarantine works is a very direct consequence of the germ theory of disease.
You don't have to understand every detail about the virus to know that keeping infected people away from uninfected people halts its spread.
Quarantine measures have been incredibly effective in countries that have implemented them seriously. China, Australia, New Zealand, Vietnam and other countries have essentially eliminated the virus within their borders. Quarantine is low-tech but effective.
Part of the problem is that quarantine means different things to different people and places. North American and European quarantine seems to have been almost entirely ineffective. Too loose to help and too invasive to not hurt.
It's hard to prove anything, especially because my government's policy is specifically not to tell us where people are infected, city, store, or class of activity, nor infections by capita, etc.
Here they ban playing tennis on outdoor tennis courts (but not other exercise usage of the court, such as weight lifting and dancercize - both of which I've seen there during Covid) while allowing people to sit near each other at the bar and drink. There's a chance that tennis balls are that much more infectious, but it seems likely that political issues got in the way of proper medical advice...
Also, leaving supermarkets open as opposed to totally roadside pickup probably wasted most of the effect of closing everything else. And failing to properly compensate small businesses led to many breaking the rules and going back early just to be able to eat.
So I think people in some places do have a good excuse to be mad about the manipulation. If my government locks me down I want to know that they really think it'll fix something and when I look at other governments versus my own, I don't get that feeling.
The problem isn't government tyranny. If half of the population decides it isn't safe to eat out at restaurants, then it won't make sense for restaurants to be open. Businesses and events are built on an assumption of a certain number of customers. If X% of the population decides to opt out of social life then it doesn't make sense for them to be open in the same way as before, government mandate or not.
You can't go to a birthday party by yourself. Even if you're fully vaccinated or don't believe that the virus exists. As long as the public perception was that people should stay home you would get essentially the same outcome, no matter what the government did.
Sure it happens naturally though, if suddenly people stop coming to your restaurant or bar and you can’t maintain it anymore, but that’s a different thing entirely from the government forcing you out of business.
You are suppose to be free to move around and assemble, period. The idea that the governor or the mayor can just destroy an entire industry for the sake of another industry is pretty fucking bad. They caused waaaay more harm than good, and in many ways we haven’t fully seen yet.
> No amount of “but people could die” can justify this, that’s an irrelevant point, because there never a time when it was proper to remove autonomy for such a reason!
Would you be interested in allowing unregulated tobacco adverts and smoking in any public spaces again as well?
I think making an addicting product and getting people hooked on it is another topic all together. Smoking is something you should be able to do, and not to do. If you are unable to move about without inhaling smoke that is injected into the scene by someone else it’s an active scenario. Getting sick is part of life, viruses and bacteria don’t have morals. You shouldn’t smoke around people who don’t want to smell it just like you shouldn’t set someone’s yard on fire. But literally controlling the movement and assembly of people because of microscopic organisms that have existed for millennia? That’s totally absurd and wholly different than intentionally burning chemical laden plant material around others.
Shutting down all of society with a very little proof ..versus a small targeted change like a speed limit or tobacco restriction that both have pretty much scientific consensus and decades of proof.
> I think that it’s almost more terrifying than the thing itself that more people aren’t mostly incredibly disturbed by the insane violations of privacy and speech.
Exactly this. I find myself very lucky to have avoided authoritarian measures by living in Japan, but I feel very sorry for my home country which multiplied freedom violations after violations. I find it very scary that nobody complained about it, despite the fact the lockdowns and curfews were stronger than any measures taken under Nazi German occupation. If the disease was actually very deadly I would understand, but in the covid case once the data were out after a few months, it was clear that elderly and obese persons were the only real at risk group. It thus make no sense to destroy economy, social, work and education lives of millions of people for this. And again, lot of countries dealt with it without heavy liberty privations and did fine (Japan, South Korea, Taiwan come to mind).
> I find it very scary that nobody complained about it, despite the fact the lockdowns and curfews were stronger than any measures taken under Nazi German occupation.
This isn't your main point, but I'd just like to point out that that comparison is... wrong, to put it mildly. Under Nazi Germany occupation, large populations were put into an effective prison, severely underfed, forced into labor, and, sometimes, just killed outright.
Even the most "authoritarian" actions taken are nothing like Nazi occupation.
I would like to understand how parent thinks our current situation is anything like Nazi Germany. It's bizarre.
I assume they are angry and feel wronged. Do they know the comparison is flawed but just want to make a point? Do they have superficial knowledge of the Holocaust? Do they think it could not happen to them?
Of course plenty of people complained about it and refused to give up their freedoms. Many states with Republican governors either refused to impose any mandates, or imposed very few that were never enforced. Democratic states, which generate a huge chunk of the money (and tax revenues), imposed draconian measures that essentially killed off thousands of small businesses and left millions unemployed. It's no coincidence that public schools in many of these states (CA notably; NY has succeeded in running public schools in-person for many students) completely abdicated their responsibility towards their students, shutting down in-person learning for the entire school year. Note that the 'follow the science' crowd is curiously silent on this: the CDC and the American Academy of Pediatrics emphatically argued against this injustice perpetrated on children to no avail.
The children who suffered from this, and stand to continue suffering because of this even after the pandemic ends for most adults, will bear the cost for generations to come. Not only will they inherit a heavily indebted country, they will also be woefully unequipped for it because of the major hole this abdication of responsibility has blown in a critical period of their lives. Two years is a huge amount of time in a young child's life, and the callous indifference to their future shown by Democratic politicians (who draw the majority of their support from teachers unions, among other public employee unions) is just sickening.
I sincerely hope that parents will wake up to the insidious damage public employee unions are doing, and move en masse to private schools or direct student funding for schools that they can choose, as a result of all this. Teachers unions have shown themselves to be completely unaccountable to the public and deserve their comeuppance.
The major variants of this virus very one of them has been confirmed to be affected by the vaccines. Even in the cases where a vaccine is less effective against a variant, the prevention of serious illness/hospitalization is always near 100%.
What I don't understand is this: with tens of millions of people already vaccinated, why aren't we seeing a huge drive to collect plasma from vaccinated people with high level of antibodies? In the early days of the pandemic (about 1 year ago), I remember China sent a large amount of plasma to Italy.
Why can't the US do the same now? The US is sitting on millions of AstraZeneca vaccines (that are not even approvad by the FDA), and doesn't want to share. How about sending plasma?
The United States has administered 2.3 million vaccination doses.
Oh, lol no, not cumulatively. I mean Yesterday. We administered 2.3 million doses in about 14 daytime hours on March 12th.
Naturally, the number of vaccinated individuals grows every day. That's what vaccinations do. But the number of doses we are administering every day is growing every day. One week ago, on March 8th, we administered about 2.05 million.
There's no point to harvesting plasma. Why would we, as a society, try to do that on any meaningful scale when we have working vaccines, produced and administered on a global scale that humanity has in our entire history as a species never before reached?
People give Trump shit for his statement that, one day, the virus will just magically disappear. He deserves it, but not because it won't disappear; it will disappear, but it won't be because of magic. The effort that the Trump administration, the Biden Administration, Project Warp Speed, the CDC, and other Federal and State Health Agencies, have put into this is something that, in 100 years, our history books will write paragraphs about. Its invisible to most of us. We still feel the legitimate and necessary fear that kept people isolated and society going over the past year. That fear isn't forever; the US was hard-hit, but the US will be one of the first countries back to normalcy, and the rest of the world will quickly follow.
>US will be one of the first countries back to normalcy
I live in Australia. The country has been to normal for a long time now, and my state specifically had a lockdown at the start of the pandemic, and since August 2020, we have not had a major lock down (except for one week in Jan 2021 due to a outbreak scare) and have been living in normalcy since then.
Just saying because it seems like people erasing and forgetting history that somehow America is the first out of this. No, many countries have done fairly well and have managed to be relatively normal.
Restrictions remain on large gatherings in Australia, with capacity limits. Most of Australia has regulations regarding social distancing. Australian cities are locked-down when a single case is detected. You mentioned the last lock-down in your city was as recent as January.
There are currently ~40,000 Australian citizens registered with the government who are trying to get back to Australia, receiving little to no assistance.
Flights are restricted into the country.
Australian citizens are banned from leaving the country.
And, the ironic thing is, in much of the US life is actually back to a very near normality. People get sick. People are dying. Restaurants/bars in some states are fully open, others are closed, others are at 50%, it just depends. Large events aren't really happening, though for differing reasons (meaning, I don't think right now its because people wouldn't attend; in some locations its because of regulation, in others its more likely just public image of the event-holder).
We went out to a bar in a state capital on Sunday, just to sit outside and get some food and drinks. I went inside to use the restroom, and you literally would not think there's a pandemic. Fifty to sixty people, probably 120% capacity (our city is at 50% capacity on bars; they don't care). No one wearing masks. Someone had their year old baby with them (also, definitely not allowed even outside covid). This wasn't a bar in the middle of nowhere, it was in the middle of a city of millions of people.
Normalcy means different things to different people and in different places. When I say the US will be first back to normalcy, it isn't because we'll be the first country with no cases, or everyone vaccinated (though, our vaccination numbers are insane); its because the people and the government just care less. For many people, nothing has changed; the world has changed a bit around them, but for better or worse (read: for worse) life already is "normal". And, for even far, far more people, like me, the only part of life that isn't "normal" yet is that I throw on a mask when I go in the store or to work. There's plenty of places around the world where that WAS their normal even before covid.
The majority of the US is not NYC/LA/Seattle/SF. It dominates the externally facing image, but its a far more nuanced and complex situation than what is happening in the major cities.
Back to normal except for any unrestricted travel in or out of the country. Isn’t there a massive backlog of Australian citizens who have yet to be able to return?
I guess you could say there's a difference. Both Australia and New Zealand have returned to normal because of success in controlling the virus. Both countries have low double digit counts of infections per day (and teetering on single digits). So I guess you could say the US will be the first to get back to normal while there continues to be a high number of cases.
> the US was hard-hit, but the US will be one of the first countries back to normalcy, and the rest of the world will quickly follow.
Though I very much like this optimistic take, this is a bit revisionist.
Specifically, Hong Kong, Vietnam, Taiwan, Australia, Japan, South Korea, New Zealand and a few others (including parts of mainland China) have already returned to “normalcy” in that their economies are growing and that all have high public confidence that contagion has been controlled.
Really like the last part of your comment. the fact that (collectively) we created, tested, released, and are now distributing vaccines in less than a year is an incredible achievement.
The US has bought its way out of the pandemic by funding the pharma companies and reserving doses.
This was a smart play, of course, and ultimately the deciding factor, but this success is only being realized after a long string of failures and ongoing inefficiencies.
> People give Trump shit for his statement that, one day, the virus will just magically disappear. He deserves it, but not because it won't disappear; it will disappear, but it won't be because of magic.
The "magic" part, I think, was about perception: Infection rates have been dropping almost worldwide for two months (more, in some places), but people seem to think infections are steady or still increasing despite vaccinations (concern about variants, old messaging (we still have signs up from November here), etc). For a lot of people, it will look like magic when it's suddenly no longer a concern.
I believe the efficacy of convalescent plasma has been shown to be minimal to non-existent, so I agree it isn't likely worth harvesting. If it were effective though, it would absolutely be worth it, because the United States isn't the whole world. There won't be enough vaccines to fully vaccinate the global population for many months at the least - probably at least a year. If we had an effective treatment that could be donated to countries not fortunate to have an abundance of vaccine doses, it would clearly be the moral thing to do.
So far convalescent serum treatment using plasma donated by recovered COVID-19 patients hasn't been very effective. There were high hopes for this treatment at the beginning of the pandemic but so far study results have been disappointing. I doubt that serum from vaccinated people would be any more effective.
The FDA won't allow convalescent plasma collection from vaccinated people (https://www.fda.gov/regulatory-information/search-fda-guidan...), on the grounds that their antibody response might be different than the response from a natural infection. (I don't know enough to judge whether or not this could be expected to cause practical issues.)
Perhaps they could make some allowances like they did with the vaccine approval method. Wasn’t the fastest vaccine ever previously a 4+ year endeavor with animal testing?
Vaccines and plasma serve 2 different purposes. A vaccine will provide long term protection, but do nothing to help a patient who is sick now [0]. In contrast, plasma will help a patient who is infected now, but provide no long term protection.
[0] Or, at least, the Covid vaccine has not been proven to do anything to help a patient who is sick now. There are cases (such as rabies) where getting vaccinated after being infected is still beneficial.
Right, but are all vaccines equal ? Take the chinese Sinovac one for instance, which several countries have been using for their mass vaccination program. Preliminary data in Brazil showed an efficacy of about 50% in preventing asymptomatic infection[1].
Are we sure that it will be able to "end the pandemic" in these countries as well as the mRNA ones? I remain a bit skeptical. In a CDC simulation[0] back in June 2020, the conclusion was that:
> This study found that the vaccine has to have an efficacy of at least 70% to prevent an epidemic and of at least 80% to largely extinguish an epidemic without any other measures (e.g., social distancing).
Could someone more educated than me in the matter chime in?
“As of December 16, 2020, there were 12,396 health workers over 18 years old enrolled. A total of 253 positive cases were collected during the observation period. After 14 days following vaccination with 2 doses of vaccine following a 0, 14 day schedule, the efficacy rate against diseases caused by COVID-19 was 50.65% for all cases, 83.70% for cases requiring medical treatment, and 100.00% for hospitalized, severe, and fatal cases.”
The near 100% efficacy against hospitalization and severe disease is still sufficient to end the disease burden of the pandemic.
The virus may become endemic to the human race, but if the disease burden is somewhere in between the common cold and seasonal influenza then the _pandemic_ is over.
Viruses evolve but so do the vaccines. I think we have about 200 more in development. I'm kind of optimistic on that front - as tech improves we'll outpace nature.
Yeah, but viruses evolve faster and branch out. Again, you make all your conclusions based on our experience with DNA viruses - this is an RNA viruses, things are different. Imagine the flu as we know it only more contagious and more lethal. How can we be optimistic when even the flu kids enough and damages the economy already and vaccines have spotty success against it.
Yeah I make it a point to never trust the opinion of "experts" on such matters which can potentially create panic in society. It's just far easier to sound assuring than tell the naked truth as it is.
Most of these experts earlier said that the UK variant was nothing to worry about. Now we know it not only spreads faster but is also much deadlier. Same thing might happen here.
Here in the UK we've already been warned that the new Brazilian variant is unlikely to be stopped by vaccines. It's surprising to see this story pop up all of a sudden.
Unfortunately, at least in the US, the massively increased buy-in to conspiracy theories got together with the anti-vaxxer movement and had a three-way with folks who still believe COVID is a liberal attack on Trump, and their newborn baby is significant resistance to getting vaccinated by a large portion of the population.
OT: Imagine "experts" from our industry explain the mainstream our world: e.g. what's the right programming language, or database technology, why types matter, or not?
Because software development is a skilled trade, not a science. The consortium discussed in the article is made up of actual scientists who do actual science.
"I am surrounded by bullshitters therefore all fields are equally deep in it" is not a correct view.
Then take data science or deep learning which is a science as sophisticated, same there.
We trust experts from other industries so much that we do not tolerate any other view without having a clue what is going on ourselves. The reason is simple, we have our views, they are political and we refer to "experts" to make our views scientific. Just my opinion and I bet that a huge number will disagree again with this comment. But—could I be right? Why not admit that I might be right? Because it's a political topic and your opinion is set.
False claims. There're as many who do and do you know what it does not matter for this discussion because data science and deep learning is a science independently of what some people do or not. This was the point.
Haha sure, read some papers about Bert and its successors. Come back and summarize what you have learned. But your comments shows so clearly that your opinion is set and politely you should check out data science and deep learning before you again write such shallow dismissals (which is against the guidelines btw).
Because no two fields are alike? We don't do anything even remotely scientifically in this industry because it's one of the few where we don't need to for various reasons
I've always thought that true engineering is anything that involves human lives. Bridges, pipes, roads, pace makers, space ships, rockets. Websites don't kill people, it ain't engineering.
That doesn't sound right. Most applications of electronic engineering are not safety-critical, unless we count requirements such as avoiding improper use of toxic chemicals, but setting the bar that low would mean just about any physical undertaking counts as safety-critical.
Projects like the Linux kernel, or the HotSpot and LLVM compiler systems, presumably count as engineering. Building a new GPU presumably counts as engineering. These systems aren't intended for safety-critical use, though.
Another example: it still counts as aeronautical engineering even if you're building an unmanned drone that only ever flies in a lab.
But do you mean: so-called experts? As in, not experts? Well, then that's just a question of finding the real ones, if they exist.
Or do you dislike how they oversimplify when talking to the public? I do too. All nuance is erased. The trick, then, is find out what (true, non-politized) experts say to each other when the public isn't listening.
Problem is that most people don't listen and turned off their brain. Look at this thread. They rather believe some random experts and news outlets calling some random dudes with random degrees experts because they have themselves no clue, never lead always followed others. What do we expect?
Which other pandemic do you think is even remotely comparable to Covid-19? (All pandemics with a comparable transmission rate happened in times that simply aren't comparable to the modern world in terms of mobility, which obviously affects the way this goes.)
COVID is different because it is occurring against a backdrop of extremely aged and obese populations, in a year (2020) which followed a weak flu season (2019), and in an election year in the USA (2020) where all health decision were heavily politicised.
"In Sweden, the observed increase in all-cause mortality during Covid-19 was partly due to a lower than expected mortality preceding the epidemic and the observed excess mortality, was followed by a lower than expected mortality after the first Covid-19 wave. This may suggest mortality displacement."
Despite their hands-off measures legally, Swedes still socially distanced aggressively. The government has been encouraging people there to take active measures in a manner unlike during swine flu. So we are still comparing the spread, and damage from spread, of a virus where significant behavioural change/mitigation efforts were made, against a virus with significantly less efforts to mitigate it.
Except when discussing poor results in Sweden, then its because they congregated, held events and allowed the virus to spread. I’m not buying either of these no true swedesman arguments.
There's nothing to buy. Data exists for this. Go check out Google's data on people's movements. It went down in Sweden significantly. Maybe less than elsewhere, and that's a rabbit hole you can get lost in. But I think the point stands that it is not a one to one comparison.
You are correct. The pandemic may end after about 20-30 months, but this novel coronavirus will stick around. It is going to be a community virus, such as the Spanish flu turned into seasonal influenza. People pushed back hard against the experts when they started talking about preparing for herd immunity and 70%+ infected. So, this messaging has become more careful.
A few months later the debate will turn to this being leaky vaccines (vaccinated still shed virus, but may not get really sick). Officially, this is also: We just don't know, we are monitoring it. But all the monkeys showed shedding. Trial participants showed shedding. This is a leaky vaccine. What happened to the targeted disease, when we used a leaky vaccine in life stock can be read here: https://en.wikipedia.org/wiki/Marek%27s_disease
Edit: I'd like a single expert predicting that our current vaccines will eradicate novel coronavirus. That would prove the downvoted post wrong. You'll find many experts agreeing that novel coronavirus is going to mutate and live among humans for a long long time after the crisis is over. Facts, people.
It's the first time we have mRNA vaccines available, which makes it much easier to update / mix different variations of the virus than earlier technologies. The mass production is still not optimized, but at least the incentives are huge at this point.
> A few months later the debate will turn to this being leaky vaccines
Made a bit more complicated by the fact that not all vaccines have the same properties here...somehow seems the mRNA vaccines do better at preventing shedding than the adenovirus-based ones [0].
Made way more complicated that it basically depends on what China did to restart Wuhan or Russia did to push through Sputnik (How much did these vaccines shed? Poor answers right now!). All of America can be mRNA while SARS-nCov keeps evolving elsewhere, just one flight away importing it. Surefire way to get vaccinated though :)
> Under normal conditions, highly virulent strains of the virus are not selected. A highly virulent strain would kill the host before the virus would have an opportunity to transmit to other potential hosts and replicate. Thus, less virulent strains are selected. These strains are virulent enough to induce symptoms but not enough to kill the host, allowing further transmission. However, the leaky vaccine changes this evolutionary pressure and permits the evolution of highly virulent strains.[12] The vaccine's inability to prevent infection and transmission allows the spread of highly virulent strains among vaccinated chickens. The fitness of the more virulent strains are increased by the vaccine.
(...)
> Highly virulent strains have been selected to the point that any chicken that is unvaccinated will die if infected. Other leaky vaccines are commonly used in agriculture. One vaccine in particular is the vaccine for avian influenza. Leaky vaccine use for avian influenza can select for virulent strains which could potentially be transmitted to humans.[13]
I never heard this discussed as a big "risk". As far as I know this was always more or less known to be the endgame and not even a dangerous outcome but the "good" scenario.
Once it's an established coronavirus, it can be like the other known human coronaviruses we already have. The reason you don't die from OC43 at age 75 now is because you probably cought it a few times before that. It's not necessarily because OC43 doesn't have a high IFR at high ages. We don't know that because we don't have a large sample of it. For all we know, one or more of the existing HCOVs may have been quite a deadly disease back when it entered the population.
We aren't going to exterminate SARS-COV2. Especially obvious since it's not limited to humans (present in mink, cats, primates, ...). And that's not going to be a big problem.
> I never heard this discussed as a big "risk". As far as I know this was always more or less known to be the endgame and not even a dangerous outcome but the "good" scenario.
The endgame is for the virus to turn into a community virus. This is not the big "risk". The big risk is in using leaky vaccines to combat the mortality and morbidity until we get there (or can reset economy). In chickens, use of leaky vaccines lead to the evolution of a disease which kills nearly all non-vaccinated. That's nothing like the seasonal flu (which would be a "good" outcome, indeed).
> Vaccines have saved millions of human lives, but according to evolutionary biologist Andrew Read they sometimes may also cause pathogens to turn deadlier. Read first put forward the theory 15 years ago. Now, in a new paper, he presents evidence that that is what happened with the virus causing Marek's disease, an infectious disease in chickens. Read acknowledges that the effect has never been seen with human vaccines, but he argues that future vaccines that prevent disease rather than infection could have the same effect. Other researchers say that no general conclusions should be drawn from the paper. Even if he turns out to be right, the study offers no support whatsoever for those who oppose vaccination, Read stresses. If "leaky" vaccines are proven safe and effective, they should be used, he says, but perhaps with closer monitoring and additional measures to reduce transmission, such as bed nets for malaria.
And for all the solid risk management in the West, China, a country where:
- SARS-1 leaked twice from a lab,
- which re-sentences Australian citizens to a death penalty as diplomatic punishment for Australia wanting joint investigation into the origin of a disease with still unknown zoonotic basis
- which would not allow WHO full access, and put information blackout its scientists
- informed the world way too late of an upcoming pandemic, pressuring the WHO to geopolitics and trade instead of world health.
That country will vaccinate a billion people with a leaky vaccine that skipped a trial with a poorly estimated 50.5% efficiency. Risky as all-living hell.
> Under normal conditions, highly virulent strains of the virus are not selected. A highly virulent strain would kill the host before the virus would have an opportunity to transmit to other potential hosts and replicate. Thus, less virulent strains are selected.
This is not correct. What is selected against is deadliness, which is not correctly referred to as "virulence."
By example, the virulence of the kind of herpes that most Americans call "cold sores" is off the charts: you can get it from a single kiss. But because the host barely notices, it's not a big deal.
Similarly, a great number of diseases occur to AIDS patients because they're omnipresent, but cause no harm in normal conditions.
Don't even get me started on mononucleosis.
And then, of course, this is just a generalization; measles and many kinds of meningitis are ridiculously virulent, as well as extremely deadly.
The response to Covid has also been night-and-day compared to AIDS - e.g. Trump was - I would argue - criminally negligent and disrespectful to the victims, but the Reagan admin were cracking jokes about it for example.
It's crazy to think about how HIV has killed some ~32 million people, and yet we rarely hear about it anymore. COVID probably won't even hit 4 million deaths (barring some much deadlier variant that we can't easily produce a new vaccine for).
Right, I don't mean to downplay the severity of COVID at all. It's just interesting that we generally don't hear a lot about HIV/AIDS anymore, even though there were still 690,000 deaths associated with it in 2019.
I also realize that probably depends largely on where you live.
The treatments for HIV are incredibly effective, if you can afford them. It can even reduce your viral load to undetectable. There is a campaign that Undetectable=Untransmittable, to reduce the stigma associated with it. I have to admit I don't know if I'm comfortable with having unprotected sex with someone who had the virus, but the data says it's safe.
There is also pre exposure prophylaxis, which isn't a vaccine but does dramatically reduce the risk.
Between the two, the disease just isn't the problem it used to be -- assuming you can afford it. In poor counties it's still a problem.
HIV is not a proximity transmissible disease so the reality is it's well controlled anywhere you've managed to get the use of barrier contraception methods into widespread adoption.
And at the end of the day if it can't spread through casual contact then it's impact on wider society will be limited once it's understood.
> I also realize that probably depends largely on where you live.
Yeah, I think this can largely be explained by the usual tendency to focus on our own backyards. Google says 'nearly 13,000 people with AIDS in the United States die each year', and I assume the rate is similar in other wealthy countries. Even if we assume the full total is causally attributable to AIDS, that's significantly less than the usual toll from flu, which we also tend to treat rather casually (which isn't to say that we should).
HIV is only transmitted during the exchange of bodily fluids.
Beyond that, we learned to treat it extremely effectively, today if someone who is HIV-positive adheres to their antiretroviral therapy they have a normal life expectancy.
With PReP and PEP HIV is preventable, containable, manageable and no longer leads to AIDS and death. It’s just a chronic infection with no health effects. Is it really still considered an ongoing pandemic?
Yes, because it continues to spread widely and access to treatment, let alone PReP, is extremely uneven across the world.
Both PReP and antivirals are also not easy. You don't just get a shot and not worry about HIV for a few years, you have to take a pill every day as long as you're sexually active, and then treatment antivirals are expensive and need to be used consistently as well. One person slipping up can mean a lot of people catch it. Even assuming you know you have it to begin with, which is often not obvious until you've been a carrier for a while.
Never mind religious groups going around vilifying condoms doesn't help.
It's getting better, but yes it is still considered a global pandemic.
I mean, it's not the same thing as COVID but like COVID it carries with it its own unique challenges and at no point has the world dumped billions of dollars into single-use vaccines for it like we've done with COVID. Its stigma has migrated (or compounded) from a "gay disease" to an "african disease".
Honestly, I really hope that one silver lining out of all this is that an mRNA vaccine for HIV might get some development now. There was some work that way before everything got diverted to COVID and now that tech has proven itself so...
If taking a pill to protect your own life every day is too much hard work we are doomed. But we aren’t, as PReP both protects people from infecting others as well as getting infected themselves.
So no, an infection does not require one person to slip up. For an infection to occur requires both persons to slip up.
Getting PReP requires regular HIV tests so it is in fact obvious that you are infected, if you get infected.
Of course this indeed only solves the issue in the developed world that can pay for (and wants to use) this medication but there really is no way around that. People that don’t want or can’t pay for this medication won’t want and be able to pay for a vaccine either.
Maybe China can help with a cite. They did have a 5-6 month head start and first encountered: brain-blood barrier pass, blood cloths and brain/lung aneurisms, reinfection, patient 0, airborne COVID, effect of mask wearing, pets getting infected, and more.
Too bad they don't allow the WHO full access to investigate, nor share critical information with the rest of the world, now suffering thousands of deaths. Most likely is a lab leak accident (Israel, UK, and US all said as much!). But unfortunately, the "China Virus" has become a political issue, and you won't find cites in the popular media anymore. Just articles about xenophobic conspiracy theories, and to listen to health experts when they tell you masks are not protective, go eat at China Town to show your support, don't worry about losing weight, and that vitamin D deficiency is a hoax.
If we're lucky the virus mutates into a very transmissible but not very symptomatic or damaging to humans variant. It's speculated that's how the 1918 flu pandemic eventually ended.
That’s true, but before that happened it appears to have mutated into a considerably more virulent and deadly form that dominated in the second wave. COVID probably would eventually burn itself out into a less lethal form, but there’s no telling how long or rocky the road to that could be.
>In developing its COVID-19 Scenarios Project, the ISC has consulted with WHO and the UN Office for Disaster Risk Reduction. The ISC has established in February, 2021, a multidisciplinary Oversight Panel made up of globally representative world experts in relevant disciplines to work with a technical team to produce the scenario map. The Oversight Panel will report within 6–8 months to the global community on the possible COVID-19 scenarios that lie ahead over the next 3–5 years, and on the choices that could be made by governments, agencies, and citizens to provide a pathway to an optimistic outcome for the world.
> it might take several more years for things to go back to somewhat normal.
People always make statements like this, but nobody defines what "normal" actually means. Some things will probably never go back to the way they were. Does that mean things won't be "normal"?
Normal also means entirely different things for different countries and different individuals. That's why I dislike statements like this, unless there's at least an attempt to define what you mean by "normal".
For all of those, you’re probably looking at 2022. For some - enough that it feels much more like normal than it has in over a year - the middle of summer seems like a safe bet for most of the US.
Where I am those are already gone. It is already "normal". There is still a lot of voluntary mask wearing, and the social pressure that comes with that, so not completely normal, and I'd still be subject to travel restrictions, but those two weren't in my definition.
I think it will be a lot sooner than you think, because it's already happening in a lot of places.
If normal just means you get to hug your grandmother who lives an hour away it might be safe right now (in a bunch of countries) or permitted but perhaps unwise (in a lot more countries) and it's likely that for most HN readers it will become a reasonable thing to do around mid-2021.
If it means snogging random strangers at a crowded nightclub after a night of drinking that is safe in a very few places (only a handful of countries with elimination or close enough have "crowded nightclubs" in the first place, those aren't a thing on tiny Pacific islands many of which are COVID free) and legal but unwise in some parts of the world right now but it might not be a reasonable thing to do until late 2021 or after for most of us.
If it means spending a week on safari in some poor country to see exotic wildlife, that likely will not be a reasonable thing to do until at least 2022 and maybe later, it may be technically safe for you earlier, but it probably needlessly exposes the locals to a virus they have yet to receive immunisation for so you shouldn't do it.
> "If it means snogging random strangers ... might not be a reasonable thing to do until late 2021 or after for most of us"
7000 people ages 18-39 have dies of covid19 in the U.S. [0][1]. There's at least 75 million people in that age group! (maybe more, sorry no handy/easy/exact reference)
That's 1 in 10,000 odds of dying for that age group. They are 20 times more likely to die of something else.
I think it is unreasonable that any of these people are restricting themselves out of fear. The 1 in 10,000 odds don't justify missing out on loosing the enjoyment of 1-2 in 20 years of their youth.
For those who are healthy and not old the numbers do not appear to back up the prevailing fearful narrative around this virus.
Quite a few people 18-39 have friends and family in more vulnerable age groups they can spread it to, and the "one-in-tens-of-thousands" odds are with unprecedented global mitigation measures.
"The odds are low with distancing and closed nightclubs" is a weird argument for packed nightclubs being safe.
Why did you put "one-in-tens-of-thousands" in quotes?
I looked it up, in 2019 there were 89 million 20-39 years olds in the U.S. [0], and 7000 ages 18-39 died dies of covid19 [1]. Mathematically that works out to 1 in 12,714, and would be a bit higher were 18-19 years added to the denominator. I didn't mean to exaggerate this number.
You mentioned family in vulnerable groups. Lets grant common sense, that someone who lives with their Grandparent's isn't going to go clubbing? EDIT: People need to use common sense, and they seem to, even in when they are not being forced.
I wish that we could measure the effectiveness of mitigations. This may be your strongest counterpoint. I end up extrapolating worst case numbers sometimes. I'd love to see you come up with a worst case number. I've got the feeling we could agree on a number, but still might disagree on how we react to that number.
Every weekend the beach bars near the Florida city I'm located in are busy. The majority of people are not wearing masks, sometimes almost nobody, sometimes that includes staff. Some places, with DJs and bands, are literally packed shoulder to shoulder as the night wears on. Like it was 2019 again!
I've also been in NY for part of the pandemic, and keep up with my circle there. As far as I know it's like you said, the Florida beach bar scene would not be tolerated. The rules are a bit stricter in NY, better enforced, with less exceptions, with more state backing.
So why are per capita covid19 deaths higher in NY than in Florida? Florida has 1500 deaths per million, and NY has 2500. [2]
EDIT: I was replying to your points, and don't mean to sidetrack us. Perhaps we need to back up? Do you think it is unreasonable for a young person to go clubbing under any circumstances at the moment? IS a definite 1-2+ years of restrictions worth avoiding a small possible (1/1000 at worst?) chance of harm.
> Lets grant common sense, that someone who lives with their Grandparent's isn't going to go clubbing?
Our recent history does not make me feel comfortable granting that.
> Do you think it is unreasonable for a young person to go clubbing under any circumstances at the moment?
I think it's unreasonable for local governments to permit said club to be open in the first place.
> So why are per capita covid19 deaths higher in NY than in Florida? Florida has 1500 deaths per million, and NY has 2500.
NYC got hit at the very beginning, before we'd settled on how to effectively treat, and before most of the mitigation was in place. Peaked at over a thousand deaths a day.
You bring up a valid point about NY vs. FL. NY [0] had more initial cases (initial outbreaks), Florida [1] had more over the summer (perhaps inside with a/c?), and they have been pretty much identical the last several months. I don't propose that Florida is doing better. But numerically it's hard to say they are doing worse. And there are at least some crowded nightclubs in Florida, and have been for months. I don't know of that happening in NY, I've heard of the ones there that tried getting shut down.
I'm not sure what to do with the idea of the someone who would willingly expose their Grandmother. Some grandmothers don't care. Some care a lot and won't take any chances. Most young people don't live with their grandmother's. I wouldn't go clubbing if I lived with my grandmother. When I'm visiting other people I'm sure to let them know about any recent exposure I've had, allowing them to decide if they're comfortable.
Maybe we should return to the main question of this thread, so we don't stray too far: Is it reasonable for young healthy people (who don't live with vulnerable people) to go out clubbing?
Given the numbers (7000 out of 89+ million 19-39 year olds have died in the country), my answer is still "yes!"
Another way of looking at it (for young people): Young people are 20x more likely to die of something besides covid [2]. Nobody thinks it's reasonable to hide from those other things, do they?
I'm in a different demographic, my odds aren't as good as those of an 18-39 year old, and I'm still comfortable going out and ignoring the pandemic when the urge strikes and I'll have a good time. I've paid close attention to the numbers, and only 1 in 600 people have died from this so far, tending to be older and with existing health issues. So my odds are even better than 1 in 600.
You may look at the same numbers and asses the risks differently. Everyone's entitled to their opinion, and to isolate as they see fit.
Perhaps a better way to continue this conversation would be to agree on some numbers, then discuss why we look at the numbers differently?
Virologists know a good bit about coronavirusus, and so far I haven't seen where any of their prior knowledge that has not been applicable to the covid19 coronavirus. I've been reassured by what this body of knowledge has always had to say about the dangers of retransmission, the longevity of immunity, and the immunity conferred across variants, amongst other things.
What do you mean about the illness being the result of stress and conflict? Are you saying that a covid19 is not transmitted by a coronavirus?
How does any of the above apply to the dangers faced by young people? Only 7000 out of 89 million have died so far in the U.S. That is a low number, especially compared to a couple years out of someone's lifetime. Do you pay any attention to numbers?
The denominator could be an estimate of the number of people in the group that have been infected, that would probably be a better estimate of the individual risk from getting infected than just averaging the deaths so far out over the whole group.
I believe that 1 in 10000 number is what you want it to be, the number of deaths per infection in that age group, not the number of deaths per population of that age group. 1 in 10000 infections leading to death gives us a presumably reasonably accurate likelihood of death rates if everyone in that age group were to get infected.
I used the population of that age group as the denominator.
The numbers of infected by age group are not as easy to find, and perhaps not so accurate (confirmed vs non-confirmed, etc).
I've approached this numerically since numbers started coming out of NYC last spring. It's just the way I've been comfortable estimating/qualifying the risk.
I think that I see what you mean, and that sounds fair to me. Basically that the disease may have only moved through half that population so far, if I follow your logic.
Dying is 1 in 10,000. But about 10% of people who get coronavirus have some problems for months thereafter.[1] This is not well understood. "More than a third of them hadn’t returned to their usual state of health 2 to 3 weeks after testing positive. The older the patients, the more likely they were to say they their pre–COVID-19 health hadn’t come back. But even a quarter of the youngest, those aged 18 to 34 years, said they had not yet regained their health."
There is a lot of precedent for this. For example, here's a paper talking about the flu and heart swelling: [0]
> During the Sheffield, England influenza epi- demic from 1972 to 1973, the cases of 50 consecutive patients who were initially diagnosed as mild cases and were treated on an outpatient basis were followed. Transient electrocardiogram (ECG) changes were seen in 18 patients, and long-lasting changes were seen in 5 patients.
It could be that the flu is worse than covid in this regard, the few studies I looked at were surprising/sobering. They were talking for years about "long-flu" after the 1918 pandemic.
Until we have numbers to back it up I would not make the assumption that covid is any worse or different in this regard. Conventional wisdom is that every virus that attacks the body leaves some people with long term lung, heart, and or brain damage.
The article you referenced itself references a paper that has that 10% figure, that many patients who remain unwell beyond three weeks (an example was given of a healthy 40 year old laid low, but back to moderate exercise after 12 weeks). The article you linked to mentioned that a quarter of 18-34 year olds were still affected after 2-3 weeks.
I appreciate the additional numbers, the most impactful that anyone has brought up in this thread. It doesn't change my personal equation, but I appreciate the data. The world is a dangerous place. 18-39 years olds are about 20 times more likely to die of something beside covid [1]. Life goes on.
> If it means spending a week on safari in some poor country to see exotic wildlife, that likely will not be a reasonable thing to do until at least 2022 and maybe later
But this is a problem. Wildlife conservation efforts in East Africa and Madagascar depend almost entirely on income from tourists, because state support is meagre. Already some activists on the ground in Kenya have complained that the past year with no tourists has severely impacted conservation efforts, and poaching and illegal landuse has already begun to return.
Also, public-health exhortations like yours operate on the assumption that every life must be saved. In the real world, that just isn’t the case: now that the vaccines are out, some countries will accept some degree of higher mortality in order to extract vital income from tourism. Even during this COVID year, several countries have remained open to tourists for that reason.
These articles are missing an important aspect of the vaccine: the immunity gained is non-sterilizing. [1] The vaccine stops the infection from becoming severe and spreading throughout the body, but it doesn't actually stop infection (and transmission) in the upper respiratory tract.
So we don't have any evidence showing we can achieve herd immunity even with a 100% vaccination rate (this article is wrong). The only thing we know for sure is we can dramatically reduce the severity of infection.
Beause vaccine efficacy is never 100%, some experts predict that we will see more deaths this year as we attempt to resume normal societal activities while SARS-COV-2 continues to circulate. [2] Although I think if we develop very good antibody tests and vaccines against the latest variants there should be a path towards minimizing deaths and severe complications and effectively turning this virus into a cold and effectively ending the pandemic.
> some experts predict that we will see more deaths this year as we attempt to resume normal societal activities while SARS-COV-2 continues to circulate.
Some 35 million Americans - heavily weighted towards the most vulnerable - are fully vaccinated. Unless something wild happens with variants, I think these experts are being overly negative.
I hope this is true. Do you have any studies to back this up? I see statements by government officials to this effect, but never any studies or data to back it up.
{kind=link}
{kind=link}
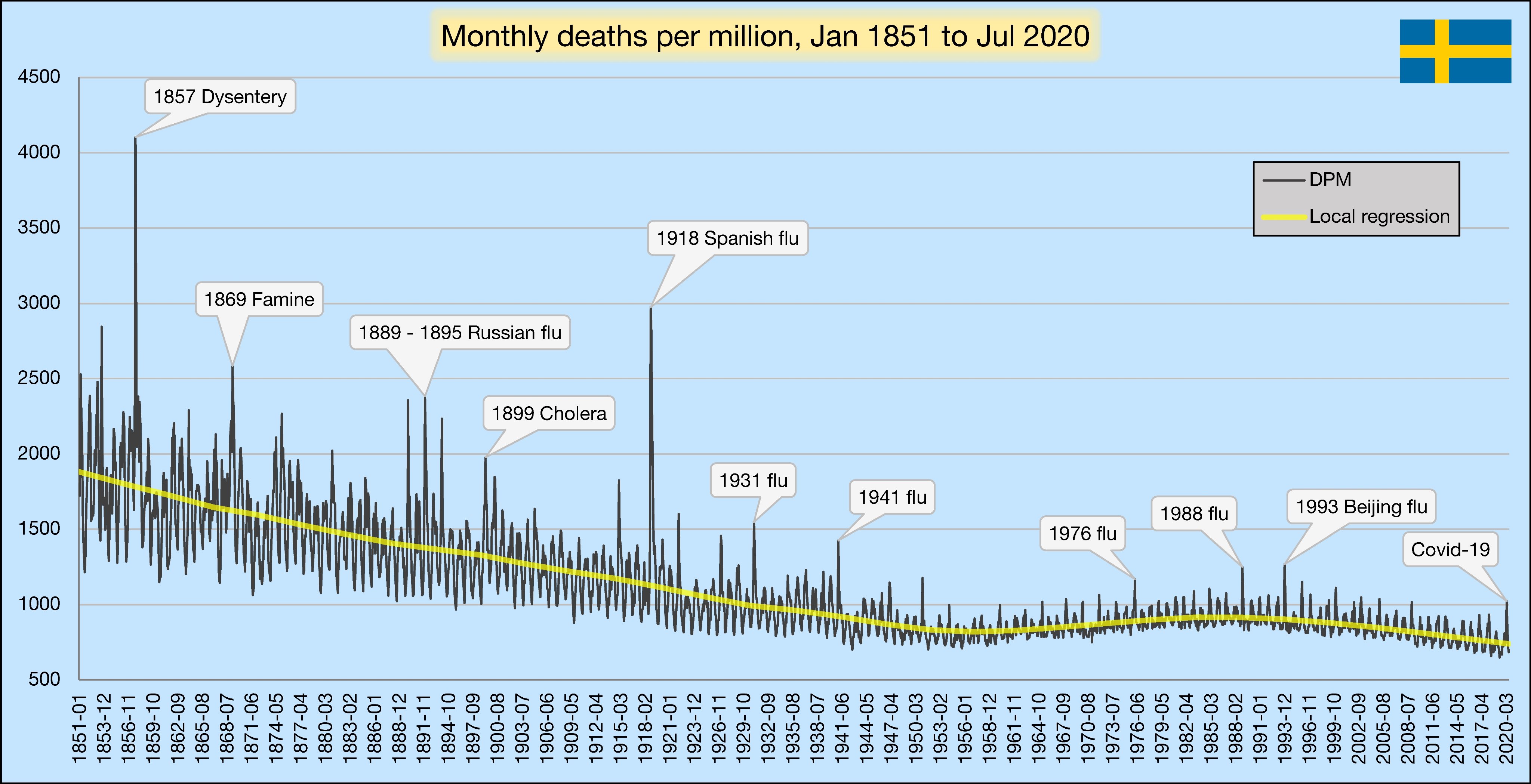{kind=link}
People with healthy immune systems, who have been exposed to SARS1 and other coronaviruses, have active T-cell defenses which recognize SARS-Cov-2 even without a vaccine.
> SARS-CoV-2 induces robust memory T cell responses in antibody-seronegative and antibody-seropositive individuals with asymptomatic or mild COVID-19, https://www.biorxiv.org/content/10.1101/2020.06.29.174888v1.... (June 2020)
> ..some people who have not been exposed to SARS-CoV-2 have preexisting reactivity to SARS-CoV-2 sequences ..previous exposure to widely circulating common cold coronaviruses might be involved .. preexisting reactivity against SARS-CoV-2 comes from memory T cells and that cross-reactive T cells can specifically recognize a SARS-CoV-2 epitope as well as the homologous epitope from a common cold coronavirus, https://science.sciencemag.org/content/370/6512/89 (Oct 2020)
Prior HN discussion on T-cells: https://hn.algolia.com/?prefix=true&query=t-cell