Health data related to Native Americans is already highly undercounted and incomplete as compared to other groups. This continued surpression of their ways of living is sad to watch. When NA’s already have little trust in Western medicine, this action by the CDC will do nothing more than erode that relationship further.
[retracted] and I hope this is just a misunderstanding. As the director of the World Health Organization (WHO) said, 2019-nCoV is a novel (new) coronavirus.[0] The CDC defines coronavirus as a virus that was not previously known — check the FAQ, “what is a novel coronavirus?”[0.5]
They changed the name of this coronavirus to reflect the disease more accurately to COVID-19.[1]
The CDC has a list of other coronavirus’ that have existed.[2]
Edit: Since there seems to be a misunderstanding from everybody’s part on this as it’s referred to as both and often interchangeably in a mainstream setting, take a look at John Hopkins guide: https://www.hopkinsguides.com/hopkins/view/Johns_Hopkins_ABX...
Excuse the incivility, but no. SARS-CoV-2 is not a strain or type of SARS-CoV. The viruses share ancestors, but SARS-CoV-2 did not come directly from SARS-CoV. SARS-CoV and SARS-CoV-2 are in the category of beta coronaviruses[0].
"The whole genome-based phylogenetic analysis presented that two Bat SARS-like CoVs (ZXC21 and ZC45) were the closest relatives of SARS-CoV-2."[1]
While we're on the topic of linguistic pedantary, strain isn't exclusive to direct mutations from a parent genome. Strains, like much of biological taxonomy, are a human abstraction to make communication of the idea of -- in this case -- "a virus sharing similar properties to coronaviruses that cause severe acute respiratory syndrome" -- albeit this is a very simplified definition for the sake of brevity.
SARS is caused by SARS-CoV-1 and COVID-19 is caused by SARS-CoV-2.
Rather, if we would like to be absolutely correct about these classifications, we would say SARS-CoV-1 and SARS-CoV-2 are both strains of SARSr-CoV (Severe accute respiratory syndrome related coronavirus), which in itself is a species, an abstract concept used to group related organisms into a convenient umbrella term.
There is no "eukaryote" organism the same way there is no "SARSr-CoV" organism. The added "r" was a recent addition when COVID-19 was discovered.
I will cede that I didn't specify this last point, and you were correct to point it out.
GP was pointing out that this was incorrect, and you just made that point by stating it yourself.
Assuming you are intending to engage in the conversation and not be a pedant, I might let you know that your replies are coming across quite coarsely. More specifically, as to prefaces on earlier comments, there is no need to excuse incivility, because there is no need for incivility here.
I found the exchange to be more than civil, with pleasantries not being taken in the literal sense.
At least this did not fall into the category of "Cold regurgitation of data" (quite popular it seems) and had a level of warmth that was an indication of passion, more than anger (from all parties).
If they added a temperature social cue to HN comments..... That would be funny.
> the previous process which was to just call a judge of a secret FISA court which no one is really allowed to know the details of.
This is simplifying the process to imply it’s nothing more than just a phone call away. I do not think any court works like that. They still have to argue their case before a judge of the court which also allows third parties to submit material in the case.
Simply saying “no one” is suppose to know about these courts is portraying this process as something unconstitutional and nothing more than a secret society of government friends. If by no one you actually mean the public, then you have a point. There’s national security concerns around these type of things that you’re ignorantly ignoring.
You act as if this court has no existed for over 40 years and under multiple administrations from both side of the aisles.
The Lee-Leahy amendment passed the Senate. Not sure how someone can say there is no counter-balancing entity with regard to FISA courts.
From Senator Mike Lee's webpage[0]:
The Lee-Leahy amendment will strengthen third-party oversight of the FISA process. Specifically, it requires FISA court judges to appoint an amicus curae (a neutral third-party observer) in any case involving a “sensitive investigative matter” so long as the FISA court does not determine it to be inappropriate.
The amendment will also empower the amicus to raise any issue with the court at any time and give both the amicus and the FISA court access to all documents and information related to the surveillance application.
It is just a phone call away. Sometimes not even a phone call. In some cases the AG can authorize surveillance and merely notify a judge and file the warrant application later (within 10 days IIRC).
Even calling it a rubber stamp is an exceedingly generous definition of probable cause.
> I still think there's a possibility this virus was already in the US before 2020.
Yeah, I don’t understand why people are so against the idea of it being in the U.S. before 2020. There’s no possible way we can trace every American who may have traveled within the China region or interacted with another person who was in that region around the start of COVID spreading. Just because there were no official cases of COVID does not mean it was not here.
I had a roommate visit Japan in November. He came back and was extremely ill for about a week. No hospitalizations but he was out of commission and isolated by himself.
I think the main evidence against it being here siginifgantly earlier is that we see how it spread when it was definitely here, so why wouldn't we have seen hot spots like Atlanta and New York earlier then?
Yeah - if someone could point me to a nursing home where 5% of the population died in a week in December/January I'd believe it - anecdotes about people being having the flu in the winter isn't the most convincing.
> if someone could point me to a nursing home where 5% of the population died in a week
Sure, if we were talking about mortality rates but we’re not. we’re simply talking about prevalence of COVID prior to the major breakout of February and beyond. These are two completely different things to be looking at.
I’ve worked in nursing homes during that time of December where people were dying. Did we think to send bloodwork off to test for some novel coronavirus? Of course not. Secondly, using the example of a nursing home as the sample population is silly as they are not the ones who were traveling. It’d be their family members and caregivers who traveled and then brought the disease into the facility.
I think you are missing the statistical point I and others are making. If the disease was introduced in a meaningful way in December/January it would be a statistical certainty we would see signs of it (such as nursing homes having huge waves of deaths or total mortality in subregions surging).
I'm not sure what your counterclaim is? There are no samples in America tested from that time period that would show that there was Covid nor is there any statistical evidence that would suggest there was Covid.
What specific evidence would you be expecting to see in December or January? The infection fatality rate for this disease is probably below 1%, and we don't know what percentage of the population is infected. We don't truly know how quickly it spreads. Nursing home populations are at greater risk, but even if the IFR is 3-5% for that cohort, the population mortality would be some fraction of that, and most of the deaths would be people with pre-existing conditions, and the deaths would be attributed to those conditions.
If there was a year-on-year increase of 1-2% in nursing home deaths for a month or two, would that register with anybody? Maybe they would have noticed if a lot of people were being put on respirators? But if no one knew about COVID they would probably just chalk that up to it being a bad flu season.
> Nursing home populations are at greater risk, but even if the IFR is 3-5% for that cohort, the population mortality would be some fraction of that,
Looking much higher than that. 80+ is 15-20% and 70-79 is 8% (https://www.worldometers.info/coronavirus/coronavirus-age-se...). It'll be concentrated more in people with pre-existing conditions so I expect nursing homes would see greater figures than that.
> Statistics from Kirkland now appear to tell the national story. Of 129 staff members, visitors and residents who got sick, all but one of the 22 who died were older residents,
So we're not talking about one or two deaths but a large proportion of your residents suddenly getting ill in the same way and of those a large proportion dying over a short period.
> Looking much higher than that. 80+ is 15-20% and 70-79 is 8%
The percentages you're citing are from the Chinese CDC [1] and represent the case fatality rate. They don't represent the infection fatality rate, let alone the overall population mortality. There's a big difference between these numbers which has been repeatedly ignored in the popular media, they keep on taking the scariest one (CFR) and presenting it in an unbalanced context. [2]
(To be fair, CFRs are the numbers we are the most certain about, but when you cherrypick the worst ones like the newspapers do they're also the scariest and least useful.)
The working definition of CFR in the Chinese study is basically people who saw a doctor, were suspected or confirmed of having COVID, and then died. But many other people would have caught the disease and not been seen by a doctor. Most of them would have been milder cases and they wouldn't have died. Key point is this number is not at all indicative of total Covid-related mortality in an exposed population.
The Kirkland story is really tragic, but it's just one data point and doesn't prove that ~15% of all nursing home populations will die. The conditions in other nursing homes could be very different, in fact that nursing home in Kirkland has since been investigated and fined $600,000 for unsafe practices [3].
Why does it have to be introduced in a “meaningful way” to be relevant? If there was at most a single case of it within the U.S. that would show that the disease spread earlier than what is assumed. Again, your argument rests solely on the idea of there must be thousands of death in order for this disease to exist within the states. That is an odd way to think about this.
It’d also be kind of hard to go back and rerun tests for people during those months, which shows why it’s very difficult to pinpoint when this disease started to really spread. I mean, if France and China both had cases during the month of November and December, you’d be hard pressed to say it’s not possible there were similar cases in the U.S albeit undiscovered.
It is not particularly unusual for a nursing home to see very high death rates around flu season. In the UK, where they have an excellent healthcare system, the average lifespan of a nursing home resident is 2.2 years.
somewhat of a dated article (2010) but the average lifespan of those admitted to nursing homes for EoLC is actually only about six months.[1]
however, some may stay longer, but then they have to worry about their condition worsening and eventually not allowing them to do ADLs (bathing, eating, dressing) on their own. the average length of stay before disablement is close to two years [2]
I understand that line of thinking but that would imply the prevalence rate of COVID was in complete parallel with the incidence rate. The former is what we do not know and that's clear when we've had patients labs reran from 2019 and found it was positive for COVID. Government data from China says the first case can be traced back to 17 November 2019 and even then they're unsure if that was patient zero[0]
How many American's were in Asia, China, or surrounding areas between October and December of 2019? How many of them were possibly infected? Nobody knows because there was no plan put in place with regard to travel to mainland China until the end of January 2020; even then since 1 January 2020, there were 430,000 people who traveled from China to the U.S.[1]
> I was hoping everyone in the US might be able to buy one.
This burst of PPE being produced in mass quantities are and were never meant to go in the hands of the general public (i.e., non healthcare workers), though. The general public does not need to be walking around with a full face shield, that’ll be a waste of materials, time and money, unfortunately.
Given that they probably would cost $1 to $5, and take almost no space to store, it wouldn't be a terrible thing for people to have a few if they want them. How many people have a $20 multi-tool that stays in a drawer somewhere? Or some bags of rice "just in case" that end up getting thrown in the trash after being forgotten about in the cabinet for 5 years?
It may not be a terrible thing if some percentage of people buy "unnecessary" Personal Protective Equipment. It creates some distributed supply in case something unexpected happens, even if under normal circumstances the equipment is unused.
It's not about the money. PPE like face shields are specifically used during procedures that involve significant bodily fluid, like intubation, which is the process of pulling or pushing a tube down a patient's esophagus. Going to to the grocery store does not require a shield.
Secondly disposable medical equipment, when used properly within a healthcare environment, is extremely wasteful. For most consumable items used in a hospital, they are covered in packaging with specific serial numbers and lot numbers that allow reconciliation if it's found that the goods are not sterile or have deficiencies. There is also a provenance or chain-of-command aspect that allows attestation of safety throughout the entire supply chain. While we might be talking about how to sterilize n95 masks, reuse face shields, and asking for donations of PPE from the public right now during a pandemic, the fact remains that in normal circumstances there is massive liabilities that hospitals and clinics would be subjected to if they started sourcing protective equipment from the public that could have been tampered with, may be slightly used and broken, or otherwise could cause harm to the patient and they'd be unable to identify the source of those resources. Everybody stocking a "handful" of PPE isn't a scalable solution to maintain a national supply.
> It's not about the money. PPE like face shields are specifically used during procedures that involve...
There is currently a global pandemic afoot that is spread by droplets expelled from people's mouth and nose. What a tool was being used for 2 months ago isn't relevant; the situation is different now.
> Everybody stocking a "handful" of PPE isn't a scalable solution to maintain a national supply.
If masks or face-shields could be cleaned fairly easily then it probably is a scalable supply. Particularly if medical professionals are allowed to supply their own work tools.
> What a tool was being used for 2 months ago isn't relevant
It is very relevant. These face shields wouldn't protect anyone from airborne/aerosol pathogens or viruses. They have a very specific purpose and that isn't one of them.
If you're talking about adapting construction grade shields (like used for painting, etc) for medical use -- sure. But you aren't going to use a face shield as a replacement for a face mask, which is what it seems like you're arguing for.
If you're saying that you should wear a face shield in public to protect yourself from aerosolized virus -- that's not the point of a face shield. The particles can travel around the sides of the mask too easily. If you want to protect from small, airborne particles, you need a mask.
Yes. Defense-in-depth. In China, most hospital red zones required 3 layers of PPE, whether that's two masks and a face shield or such. One layer alone is not very good, and a face shield alone is no good. A mask and a face shield are very good, especially for confined spaces like subways and busses where there are jerks coughing and sneezing all over without hygiene or manners.
What if I want to protect myself and my facemask from large droplets. I also want to protect myself from accidentally touching my face. Is a face shield okay then?
And if so, why not drop $300 million to get one for everyone in the US? They're cheap, wash easily, and that's less than 0.02% of the last stimulus.
If someone is facing me and a stream of airborne particles hits a plastic shield instead of streaming out to me, it seems pretty likely that I will be protected.
I'm certainly open to the idea that fluid mechanics are complicated and somehow air currents are going to do unhelpful things, but until I find someone with a paper on the topic I'd much rather be talking to someone wearing a face shield than not.
Plus obviously wearing a face shield will protect against self-inflicted infections from a contaminated finger.
And you'd be wrong. Sure, a face shield will protect you from liquid streaming out at you (partially). However, it isn't a liquid that you need to protect yourself from in this instance... it is aerosolized particles. And those travel in the air. So when you breathe in, that air can and will move around the face shield.
The sibling comment about smoke moving is exactly right. Smoke is a great example of how small particles can move and travel in the air. If you think that a face shield will protect you from something in the air, you'd be wrong.
Side note: this is how N95 masks are actually fit. (Well, not using smoke, but similar test). If you can smell the chemical used in the test, the fit is wrong.
If you really want to protect yourself from other people sneezing -- stay away from other people. That's why social distancing is still the primary, and best, recommendation.
Isn't the recommendations by many countries to wear even cloth masks (e.g. the recent reversal by the CDC) _because_ there's a good chance COVID-19 can spread via large (i.e. non-aerosolized) respiratory droplets?
(Not that it doesn't also spread in other ways, but removing even one vector would be better in this case than not doing so.)
I'm not sure why there is a recommendation to wear cloth masks in other countries (not discounting it, I just haven't looked). However, I believe that the primary rationale for the CDC switching their recommendation that everyone should wear masks has to do with the great numbers of asymptomatic carriers. In this scenario, wearing a mask is not designed to protect the wearer from others. Wearing an ill-fitting mask is not protective to the individual. Instead, wearing a mask is designed to protect others from the wearer. Because people are carriers before they exhibit symptoms (if they ever have symptoms), you can't know if you are infected or not. If you are wearing a mask, you are limiting the potential spread of virus from you. This way, you are keeping any potential virus closer to you so that others are more protected. This goes hand in hand with social distancing. If you use a mask and don't distance yourself, you aren't helping at all. I'm looking for a CDC reference, but this was also the rationale presented in local media reports.
If you're really curious, Ars Technica has a really good writeup of all of the relevant studies.
Most of the research above assumed either surgical or N95-style masks. There was one study that looked at use of cloth (non-medical, non N95) masks, and this was the key finding (from Ars, not the paper):
Wearing cloth masks resulted in significantly higher rates of infection, the authors found. They also noted that in their test, the cloth masks were only 3 percent effective at blocking particles.
Regarding everyone wearing (surgical) masks to protect others:
In a study published April 3, 2020 in Nature Medicine, researchers found that surgical masks reduced the detection of respiratory viruses in aerosols generated by infected people breathing or coughing in a breath-collecting machine.
> Wearing cloth masks resulted in significantly higher rates of infection, the authors found. They also noted that in their test, the cloth masks were only 3 percent effective at blocking particles.
Hoo boy that's misleading by itself. The control group was "use what you normally use", and had the following numbers:
> In the control arm, 170/458 (37%) used medical masks, 38/458 (8%) used cloth masks, and 245/458 (53%) used a combination of both medical and cloth masks during the study period.
Given those numbers, it's basically impossible to use this data to tell us anything about the efficacy of cloth mask vs. no mask. The control group did wear their masks less often, but it's still very unhelpful data.
> This may lead some members of the public to be lax about ... washing their hands frequently and thoroughly. Moreover, donning [a] mask may lead some people to touch their faces more, some argued.
> simply touching their mask could contaminate their hands if there are viral particles caught on the outside ... a mask wearer could then transfer virus particles from their mask to their face
So even with all the above steps that have to occur, it's still no worse than getting a face-full of Covid directly.
Almost every stupid, pointless, dangerous argument against masks boils down to:
People may not wear a mask properly.
People may not wash their hands properly.
The first one is used as an argument against masks, so why is the second not only not used as an argument against hand washing, but also used in arguments against masks?
People don't always practice social distancing. So why don't people argue against that? Oh, because that too is reserved for arguments against masks.
It's fucking ridiculous. Why do some people continue to spend so much time and effort trying to discourage use of potentially life-saving items?
You say that with great confidence and a lack of sources; and I'm guessing we are equally ignorant on the actual physics of how small droplets move.
The details aren't clear on how the virus is spreading. The virus might have multiple modes of transmission. Closing 2 of them reliably a great deal. There are important things to do with "catching COVID" that aren't binary; starting doses likely matter as well.
I'd rather not talk to you in person if you aren't going to cover your face, tyvm :)
That is something that I've been wondering about too. I work in biotech but not as a scientist. These things are tricky to nail down as they seem to be very individual specific. Theoretically, in an exponential growth model, it wouldn't matter if you were inoculated with 20000 or 200000 virons, after the incubation period post-infection, you're going to be generating a huge amount, millions and millions, of virus particles in either case. Certainly, if you keep getting exposed, you're immune system is going to get overwhelmed quickly, but for a single event, I don't think it matters.
Thanks for taking the time to post the link, but it wasn't convincing as it lacked data and other relevant scientific information that I was looking for. Personally, I do not consider the NYT to a reliable source of information, but I know many do so maybe the link will help someone else.
It increases the effective time large droplets need to spend in the air to get to me, and decreases the airflow around me. It's about the same reason plexiglass screens help, and keeping a 6-foot distance helps.
It’s okay to admit you’re wrong. It’s okay to not understand everything. It’s okay to defer to experts.
So many people on HN and in tech have the same attitude that if they just spend 5 minutes thinking about something then they can intuit an answer and that they must be right. This is a dangerous way of thinking. If anyone took what you’ve been saying as correct they’d be endangering themselves and depriving medical professionals of tools they need.
But I'm getting my opinions from the experts? See [0]. They recommend covering your face. I agree with them that cloth is more effective than a plastic shield but I'd expect a plastic shield to still be better than nothing. You've got to try and stop droplets from leaving your mouth and reaching other people.
A face shield would be better than failing to create a makeshift covering from a shirt for most people and it'd be resistant to decomposing so it could be stored long term in a home. It'd be a reasonable thing to stockpile.
I don’t think it’s reasonable to stockpile given the huge demand for them by medical professionals.
I also can’t imagine a situation where you can order and wait for a shield but don’t have the time or resources to get a surgical mask or cloth.
And obviously the shield alone isn’t going to protect you from particles. And it might not help slow the spread if you’re infected yourself.
But again I’m speculating. If the health professionals say they need them and the public doesn’t, I’ll defer to them. I’m not an expert in their field and I don’t want to pretend to be or cause anyone to think I am.
This is just common sense. Aerosolized particles are not impeded by a shield. A shield is intended to obstruct ballistic projectiles. If those projectiles are aerosolized and are in the air that you breathe, then the shield will offer no protection at all. Even an N95 mask still can let in up to 5% of these particles. What efficacy is a piece of plastic in front of your face going to do against that?
> If those projectiles are aerosolized and are in the air that you breathe
It seems like you're imagining that the mucus and saliva particles would behave like a gas, but it's a suspension of liquid particles in the air, which behaves slightly differently. Think of breathing onto glass -- a lot of the aerosol I expel adheres to the glass. Some smaller droplets may move around it, but it's still preferable to receive a smaller dose of the virus.
[I'm no microbiology expert, so obviously take this with a grain of salt :-).]
I'm not sure whether the initial dose affects the severity of the disease, but it seems clear that it at least affects the probability of infection. The individual action hypothesis [1] posits that each individual pathogen has an independent chance of infecting a host, i.e.
P(no infection | n pathogens) = P(no infection | single pathogen)^n
So if one is exposed to a single unit of the virus, infection is theoretically possible but unlikely. At higher doses infection becomes overwhelmingly likely.
I don't know how accurate the IAH model is, but there seems to be a good amount of evidence that infection rates are at least positively correlated with dose, e.g. [2].
Well there's two things. There is the 'minimum viable dose' which you can estimate for various diseases, that will most likely result in an infection. And then there is the dose size (above that minimum).
With an exponential curve, whether you start off with 10,000 or 100,000, given that it takes about 2 weeks for our adaptive immunity to kick in, the virus is going to be in the hundreds of millions in either case.
[I work in vaccines, but not as a scientist, so I'm just trying to absorb as much as possible here..]
Yeah that's fair -- there might be some high-exposure situations (like being coughed on) where infection is very likely with or without a face shield.
I suspect that a lot of airbone infections are from inhaling small doses here and there though, considering how long mucus droplets can stay suspended [1] --
> Particles of diameters 1-3 μm remained suspended almost indefinitely, 10 μm took 17 min, 20 μm took 4 min, and 100 μm took 10 s to fall to the floor.
I'm really not a medical expert at all. But, just thinking about it one could at least speculate or argue: A smaller payload means the virus takes a longer time to "become very active" in the body and delaying this "ramp up" period may give your body's immune response a longer lead time from when it first "sees" the virus to when it becomes dangerous to you.
Well with an exponential curve, even if the amount of the initial dose changes 10 fold, from 20,000 to 200,000 virons you will get to hundreds of millions in pretty much the same time. I believe adaptive immunity takes about a week or two to kick in, and in that time the virus is going to keep multiplying like crazy, regardless of the dose.
Also, suppose you were living with a partner and both of you got infected. Both of you will continually shed and "re-infect" the other, so would we expect that the infection will necessarily be severe?
> this is how N95 masks are actually fit. (Well, not using smoke, but similar test). If you can smell the chemical used in the test, the fit is wrong.
And if the smell is less strong than it would be if you weren’t wearing the mask the viral load you’ve been exposed to is smaller. You are less likely to be infected and if you are infected your immune system has more time to ramp up so you’re more likely to fight it off.
Viruses don't diffuse through the air like smoke. Viruses are contained within the aerosolised droplets of your bodily fluids that are ejected through sneezing, coughing, blowing the nose. The survival of the virus outside of the body exposed to the elements is limited. Viruses have limited lifespans and can only reproduce within the medium of the bodily fluid. Every virus has different characteristics, and may have a longer or shorter lifespan. These characteristics are more or less universal for viruses though.
It's not impossible for them to travel longer distances through the air. For the most part they are limited to the initial propulsion from the body. A better analogy would be spraying an aerosol can and watching how the droplets settle.
I think a better comparison would be to try inhaling wet steam (i.e. a suspension of liquid H2O) from behind a face shield. You'll probably inhale some, but a lot of it will adhere to the shield.
Yeah, that is pretty much what I'm imagining. If someone tried to smoke behind a facemask it seems pretty likely that most of the smoke will be caught behind the mask then drift out behind them like a comet trail, or move up/down. Only small wisps would end up traveling forward to where I'd be standing for conversation. The doses of virus would be diluted very rapidly which is helpful.
Ideal scenario would be most of the smoke gets pushed down in a knee-wards direction, which is well within the realm of the imaginable.
>If someone tried to smoke behind a facemask it seems pretty likely that most of the smoke will be caught behind the mask then drift out behind them like a comet trail, or move up/down. Only small wisps would end up traveling forward to where I'd be standing for conversation.
You ARE the person in the faceshield (I assume you meant that instead of facemask), you don't control what other people do so assume they uncovered. The smoke is in the air, it can reach you. Will it get around that shield or not?
How could me wearing a face shield help protect me from catching the virus? It'd be mostly useless; although obviously as mentioned it'd stop me touching my face as much as normal.
This is all about containing the spread.
Although I suppose in hindsight that explains why people were downvoting me.
This is potentially misleading. Viral load is a significant factor in the seriousness of most infectious diseases. This is why you'll likely be ok if you pass a coughing TB patient in the street and inhale a few bacteria, but are much more prone to contract TB if you spend an entire day cooped up in a small room with the same coughing, infected individual.
This is thought to be why an unexpectedly high proportion of young, healthy doctors and nurses are getting seriously ill from Covid-19. Statically, you'd expect almost all of them to get mild disease.
> There is currently a global pandemic afoot that is spread by droplets expelled from people's mouth and nose.
Do you have any source on how face shields are an effective tool against atomized covid19 viruses? The general guidance is that facial masks are effective at barring infected people from emitting contaminated particles, but not good at stopping healthy people from having contact with the virus. Therefore why would an open face shield, which filters zero, be a better solution?
That's the general guidance in countries getting overrun by COVID-19. In countries which have stopped it, everyone wears facemasks. Chinese scientists have good data that surgical masks help in both directions.
Face shields reduce flow of air around you. Think of the six foot rule, but add a few more feet. They also reduce projectile sneezes (and "say-it-don't-spray-it" talking, coughs, and even breathing) by quite a bit. Think about sneezing in your elbow, only much better.
I hear mask promoters say the “it’s to protect others from you” line, only to turn around and say “masks are obviously useful, that’s why doctors wear them.” The truth is, mask use is built on incredibly shaky evidence, so it’s no surprise that now face shields will become part of the hype. Both may indeed be useful, but without a clear model of effectiveness, it’s hard to make good assessments.
You seem to conflate so many things here. Doctors wear mulitiple types of masks. Surgical masks (as are recommended for the general public) prevent a doctor from spitting on a patient accidentally (just as they prevent an infected individual from expelling virus laden spit droplets). Surgical masks provide limited (if any) protection from airborne droplets. Rather an N95 masks (with a seal and filter) is used. To make this effective to protect the wearer, goggles must also be worn. The general public does not wear goggles. Further,training on putting on and taking off masks is provided to medical professionals. Face shields protect from yet another class of dangers (splashing of contaminated fluid). The general public has little reason to wear these.
I thought the entire point of wearing a mask was precisely because we don't have clear evidence as to it's effectiveness. With such a degree of uncertainty (we are literally in the midst of an epidemic) it's not very practical to wait around for perfect information and evidence before you act
Also, tin foil hats. You can't prove they DON'T work, can you? Even if they only add marginal protection, every bit counts. And they might, so can it hurt? This is why we are recommending tin foil hats to all Americans. That and a nice contribution from the tin foil lobby. We expect all Americans to commence procuring and constructing tin foil hats, and arguing about it on social media, and hope that this distracts them from noticing that their government is practically a failed state.
It turns out that "feeling safe" isn't the same thing as being safe, and feelings of safety will not actually effect infection rates, but Americans can't quite grasp that. And, hey, feelings of safety are about all we've got now, so.
I hope a doctor or nurse or respiratory therapist can correct me, but my layman’s impression is that intubation itself isn’t causing deaths as much as having to be intubated means you’re already in dire straits.
I was recently intubated 3 times in the last month and had no ill effects. I know that’s just an anecdote but no doctor ever told me it would be super risky. The alternative to not getting it however usually meant death.
> pulling or pushing a tube down a patient's esophagus
No, that's another procedure. Intubating respiratory patients involves targeting the trachea and avoiding the esophagus. An esophageal intubation can be Very Bad.
That said, as an early advocate for face masks for the general public, I'm in 100% agreement that face shields are pointless for the general public. We don't need them.
To go into a little more depth (I assume you'll see this given that you appear to be monitoring my threads):
You seem to have a mental model whereby any viral particle that bypasses your body's physical barriers has "won" - game over. But that's now how the immune system works. We want to minimize the viral load as much as possible, since with all known infectious organizations there's a dose-response relationship: the larger the dose, the worse the illness often is. Tiny loads are often effectively fought off my the immune system.
We this is vividly in a bacterial illness like TB. In TB, there's little risk if you pass a coughing TB patient in the hall. But if you spend the day with them in a poorly-ventilated office, your risk increases. If you live with the patient, your risk is very high.
The same principle applies with viral illnesses like Covid-19. And given that the only access route that is actively pulling viral particles into the body is the respiratory tract, it stands to reason that protecting that route has a higher payoff than protecting a lower risk route like the eyes.
That's not to say that people in high risk situations like Covid-19 wards of hospitals shouldn't cover their eyes! Obviously, they should and do. However, for most of us, the best protection we can use without using BL4 protection gear (obviously, not practical or needed for the general public) is to wear a mask. Mostly, the mask is to protect others from you, but depending on what kind of mask it is, it can also protect you from the virus.
Finally, most health authorities are now recommending that the general public wear masks. CDC changed their recommendations a week or two ago to recommend wearing masks. As usual, the WHO is moving slowly as large bureaucracies often do, but I don't doubt they'll also recommend them in the end as more evidence of their efficacy emerges.
> intubation, which is the process of pulling or pushing a tube down a patient's esophagus
Hope not. It's endotracheal intubation. Tubing the gut (accidentally) leads to gastric distention as we ventilate the patient, leads to aspiration, leads to aspiration pneumonia, leads to huge increase in morbidity.
There is a shortage right now and we are collectively trying to address that but it is strange to say that this particular product and the safety practices you describe is the "reason why we pay federal taxes".
Your more general point that having a national stockpile of <insert-critical-item-here> for disasters of various kinds is of course valid, but that is true irrespective of the particular nature of the normal use of those particular items.
And we've learned that the federal government isn't particularly good at stockpiling. I hope we can find a way to have some non-partisan after-action committees to figure out how to do better for the next disaster.
Does esophageal intubation happen much? I was intubated a month ago due to non-COVID respiratory failure. I also ended up getting pneumonia but no one knows when I got it. If that happened to me would my medical team have told me? Speaking generally obviously since you don’t know my case of course.
> If that happened to me would my medical team have told me?
I don't know where you are. In England healthcare professionals and their organisations have a statutory "Duty of Candour". They have to tell you when something went wrong, why it went wrong, what they're going to try to do to fix it for you, and what they're doing to prevent it happening again in future.
In general esophageal intubation results in death. The patient is not getting oxygen, and so they die. I believe esophageal intubation gets reported to the Board of Medicine and is a really big deal for the hospital and doctor involved.
"Everybody stocking a "handful" of PPE isn't a scalable solution to maintain a national supply."
No, but there's no harm in it either, and some potential benefit in case it takes a few days for the federal government to organize a response.
We all assume the government is going to make sure the food supply is maintained, but everyone is also buying some extra food just in case there's a temporary gap.
We don't need to choose just one way of preparing for the unknown.
Also, I was just saying the general public might purchase a few of these masks for themselves for their own use, not that hospitals might rely on the public for supplies.
The harm right now is that there's not even enough PPE for hospitals, so anyone buying a face shield for themselves, if that were possible, would keep a face shields from going to a health worker who needs it more.
A couple months from now, when pressure on the healthcare system is lower and manufacturing capacity is ramped up? Sure, I'm all for it.
That is a completely different situation from what I'm discussing.
I'm not talking about who should get priority for PPE right now. I'm just talking about the idea of the general public having a couple uses worth of PPE just in case. Is now the right time for them to prioritize buying PPE for themselves over hospital workers? No.
Based on a number of reports I've read about the N95 market, there seems to be plenty of PPE available domestically, but it's all being sold to foreign buyers because the government refuses to institute export controls.
For what, though? And I'm 100% being honest here, what is the specific situation you are envisioning that requires a face shield in your home?
In a medical setting, shields are typically used in conjunction with eye goggles and respirators when performing procedures that have a tendency to cause or be around splashing body fluids. Outside of someone sneezing or spitting on you directly, I can't think of an analogous situation that I come into on even a rare circumstance that a face shield would protect me from.
How about this? https://www.newsweek.com/coronavirus-gun-sales-asian-califor.... Asians don't exactly fit the traditional stereotypes for firearms purchasers but the attacks described and similar bad behavior directed at international students from Asia on college campuses certainly show that there are people out there willing to attack them based on imagined threats and therefore some level of concern by Asians for their personal safety is merited.
I notice that it's "the media are telling them that Asians are being targeted", not "Asians are buying guns because they're suffering from racist attacks". Again, the belief that people will do bad things to each other when order breaks down is much more prevalent than the actual incidence of people doing bad things to each other when order breaks down.
I'm not saying it can't happen - there are always racist assholes out there. But the media will tell one story of a racist asshole harassing an Asian family rather than 100 stories of people being genuinely nice to each other in a crisis. Because we'll click on that one bad story and ignore the 100 nice ones.
I find your dismissiveness of the idea that racist attacks against Asians could be actually be occurring to be disappointing but not surprising in members of the modern left.
I repeat, I'm not saying it doesn't happen. I am not "dismissing" racist attacks. I'm saying that media will massively over-report any such attacks, and under-report any incidences of people being nice to each other. So we end up with a belief (based on the evidence that we receive from the media) that we're going to be attacked, and not (which is the vast majority of actual interactions) that strangers will help us.
I've seen what happens when the electricity goes out and stores are forced to close - people are really nice to each other and help each other out whenever they can.
Let me put it another way: if you owned a gun, would "the electricity is out" be a reason to shoot someone?
Imagine being at the gas pump, and the person next to you sprays gasoline at you. A faceshield might keep your face from getting soaking wet, but if you smell the fumes, it hasn't prevented exposure to your sinuses or lungs.
I'm hoping Doctors aren't being hosed down with concentrated gallons of trillions and trillions of virus. PPEs aren't going to do much in that situation.
The government already has its hand in the food supply with all the farming subsidies it hands out. It can either change the subsidies to match the situation, or get heavily involved into the resource allocation as it has done in wartime.
As a good example, European agriculture is currently threatened because there are no foreign workers in the fields. The German government responded by better connecting unemployed workers to local farms, and by changing the rules to allow some foreign workers to come in.
That's just a hint of what governments are capable of. It pales in comparison to a war economy.
Stanford hospital, for example, throws away one N95 per patient doctor visit. They are not sterilizing and reusing. So my friend who works there is using many dozens of them per day. It seems like they could come up with material-preserving procedures like sterilization, but they're not.
Because best data to date is that sterilization procedures damage the mask in ways that render it unsafe.
When someone comes up with data finding a safe way to do so, the masks won’t go in the trash. In the meantime, I’d you have the masks to spare, you -should- be using them safely. Masks are pointless if you use them in a way that will get you sick.
Says something about our society, though, that doctors at Stanford can use a mask per chat "just in case", while just across the bay at Oakland Kaiser nurses are working with multiple confirmed coronavirus patients on a single mask...
It seems to me that pretty much every society has struggled to deal with this. Perhaps because it isn't something that has many reasonable direct analogues in our collective experience?
It is very easy to spot deficiencies after the fact. Much harder to spot them before.
I don't think it says that at all. You can't cherry pick two particular institutions and draw some sort of conclusion about "society". In this particular case it seems like the entire conclusion is based on nothing other than preconceived notions of what reactions "Stanford" and "Oakland" trigger in the reader. There doesn't seem to be any particular details about the actual situation at either location and how those institutions are managed.
If anything his comment reinforces negative stereotypes about the two regions. So many people in the Bay Area look down on Oakland like it’s a blighted disease-ridden wasteland and think the peninsula is some kind of haven for the rich and well off.
For reference, one of those institutions is in Palo Alto and the other is in Oakland. While Oakland has been massively gentrified it's still much more affordable to live in compared with Palo Alto.
No, THAT’s untrue. Look at your own link. You can sterilize the mask to preserve its filtration ability, but no one has shown it maintains fit. A poorly fit N95 is no protection at all, which is why hc workers get formally fit tested when starting a new gig. Which is why That link makes “no one knows what it does to fit” one of its top line bulletpoints.
There’s no plausible mechanism of action for masks under which this is true. A properly fitted N95 will block 95% of particles which is less than the kind of hazmat spacesuit with face shield and positive air pressure you’d ideally be wearing if working with someone with Ebola or similar. Maybe it really is impossible to get proper fit on a reused mask. Perhaps it’s only as good as a normal surgical mask which blocks just under 90% of virus sized particles.
Every reduction in the amount of virus that gets into your lungs makes it less likely that you’ll get infected and if infected gives your immune system more time to ramp up. That’s why people care about viral load. Running through someone’s cough is less likely to kill you than being in a small poorly ventilated room with someone coughing uncontrollably for minutes at a time.
You seem confused. This is a complicated topic. That CDC says sterilizing masks is not a safe practice, but in a crisis it's better than having no mask.
> When someone comes up with data finding a safe way to do so
There's the data and very clear recommendations by the CDC on when and how to do it. Whats' the confusing part? I don't think anyone is suggesting this approach during non-crisis times.
They're setting up one of these[0] in Boston, allowing hospitals to sterilize and reuse 80k masks / day. There's an article[1] in the Boston Globe about it, but I'm not sure what the paywall situation is there.
That line of thinking would've made sense a year ago, but the problem now is that "the unexpected happened". Now even things that cost $1-5 to manufacture can't be manufactured fast enough to meet demand (which is probably something like 100 million to 1 billion masks). If we can't get PPE to all of the healthcare workers or even most of them (and right now we can't) then there's no way they should go to the general public.
If you're not fitted and trained on the PPE you're using, it's more likely to cause harm than to provide any protection. If not direct harm, then by providing a false sense of security.
You need to not only know how to use PPE, but know what it's limitations are, and what it's designed to actually protect you from.
Wearing a shield thinking it provides any protection from an aerosolized virus is a perfect example of having the wrong expectations from a piece of equipment.
It is incredible how selfish people are. The frontline workers are desperate for any kind of PPE, but we still have random people, who are mostly staying at home, that want to get in the front of the line.
The majority of the replies from non-medical professionals here on this supposedly intelligent forum perfectly illustrates why that happens. People think they can tackle any problem and come to the correct conclusion with a minute of thinking alone, with no real knowledge or experience or testing. Now extrapolate that to the entire US or world and it is sadly not surprising that people think they know best and doctors and nurses and patients be damned.
Staying at home and limiting spread is the most effective way to help professionals.
PPE helps limit spread. The trick is to buy stuff which doesn't take away from doctors. Cotton masks. Face shields. Etc.
In contrast to nonwoven fabric, a toy factory can produce a billion face shields if you want it to. You can but them online for a buck (in quantities of 10). It ain't taking away from anyone.
Regular people should not use non-reusable anything. Just because I can spare $100 doesn’t mean I get to trash the earth with disposable junk. Make reusable/washable masks and then I don’t care if people cover their face or behind with it. Masks do help - for allergies, dust, and other things. I do wear a bandana while running because it helps with allergy. Only because I don’t want to risk another lung issue while also being in risk for covid.
What about the environmental impact of people buying everything "just in case?" Should we be stockpiling oil like crazy right now when prices are low just in case (while also artificially driving up demand)?
Isn't one of the key criticisms of farm and manufacturing subsidies that they are wasteful uses of our budget while one of the arguments in favor of them is that it maintains our infrastructure "just in case"? What about trying to buy out a foreign company to control a coronavirus vaccine or mandating that all domestic companies fulfill federal government orders before any international orders so that we have enough materials "just in case"?
My point here is that the just in case attitude for non-essential goods like PPE normalizes the same thinking in other arenas and it is unclear where we should draw the line. It is a slippery slope.
If we did more "just in case" and less "just in time" we'd be in a much better situation right now. Maybe we need a better tradeoff between efficiency and resiliency.
These don't look like 'normal' face shields that you'd find in a woodworking shop. They're just splash guards, won't stop anything remotely solid that's flying.
Face shields are more effective than masks at preventing exchange of droplets.(1) They can be cleaned and reused so it may save money and material for the general public to popularize face shields.
Right, but staying home is even more effective at preventing exchange of droplets. The face shields should be going to people who can't stay home and are forced to be around contagious people.
A huge number of Americans cannot stay home and are not healthcare workers. People have bills to pay, and not every non-healthcare business is closed, unfortunately.
It's unfortunate because these people are having to put their lives at risk, unexpectedly. They didn't ask to be on the frontlines. In addition, many of them haven't been able to get hazard pay or adequate sick pay.
And some of them (especially within those fields) may be forced by their employer to work part-time and not be eligible for employer sponsored health insurance.
You’re allowed to leave your house. Exercise, pet walking, and essential shopping and other essential activities aren’t banned. Put on a mask and go for a walk in your neighborhood and keep social distancing.
Right - this is obviously what I would do. However, if face shields were helpful for reducing risks for general interaction (no idea if they are) then I’d also want one. The fastest path to leaving the house is reducing the risk of leaving, so some simple PPE (that is more effective than a mask) would be great.
Think of it like a squirt gun. If someone is spraying a squirt gun at you, a mask will protect you a bit, but it eventually will be saturated and you'll be wet. However, if you have a face shield, the water will just roll off.
Masks are better at protecting you from small particles. Using a face shield without a mask would do you absolutely no good when you're trying to protect yourself from an airborne pathogen or micro-droplets. When you breathe, you're going to draw in air from around the sides of the shield.
If you have a mask (N95), then you're breathing air in through the filtering fibers of the mask. This is what protects you.
Masks and face shields have two very different purposes.
Yes. In January and February, we were "meant to" all keep traveling, spending, going to conferences, and parades. I'm not sure how a passive "meant to" helps. And we were all "meant to" not wear face masks, until just now.
These things are common sense. If you don't believe a face shield will help, why bother sneezing in your elbow?
We have three modes of potential transmission:
1) Large droplets, where face shields increase the effective distance from others.
2) Contact, where faceshield prevent you from accidentally touching your face.
3) Aerosol, where faceshields don't do a thing.
But reducing 2 out of 3 modes of transmission for a buck or two makes complete sense.
Several US state governments are strongly asking people to wear masks now. My local government asked so strongly they had to clarify that no, they could not prosecute you for not wearing one. And while they generally demonstrate masks that cover the nose and mouth, the earlier guidance was to avoid touching the eyes, as that was believed to be a major vector for droplet absorption.
So... how do you reconcile your statement with that?
That strong suggestion is so that a person with the virus will be wearing the mask, and therefore less likely to infect other people. That type of mask is more or less useless for protecting its wearer; its purpose is to protect everyone else.
It's very simple to just put up a full shield between the clerk and the customers, you don't need to strap the shield to people's faces when there's a static point of contact.
I had to go to the hospital today for a follow up X-ray after a month long life threatening illness. Every single desk and checkpoint inside either had the glass windows slightly cracked open but essentially closed, or they were draped in plastic covers. My pharmacy also did the same thing.
Or to wear protective gear that costs basically nothing. Not touching your face at all is extremely difficult where as wearing a mask is very simple. Why suggest very difficult measures when very simple ones work better.
>The general public does not need to be walking around with a full face shield, that’ll be a waste of materials, time and money, unfortunately.
Mostly time given current priorities -- given that we've spent 100000x the materials and money buying every kind of disposable plastic crap every year for no reason at all...
Touching one's mask is infinitely better than the alternative of touching one's face, and in the case of a non-symptomatic individual wearing a mask to reduce outbound infectious particles has no bearing at all.
The whole 'masks are too hard to use' thing was a horror perpetrated by gov't officials afraid of private individuals hoarding masks.
> Touching one's mask is infinitely better than the alternative of touching one's face
That depends entirely on if there is a viral build up on the outside of the mask.
Discouraging people from using N95 masks was specifically to avoid the private hoarding of masks.
But discouraging use of other masks (and N95) by the public is because they do not protect you if they are used wrong. When any air passed around a mask, then you are at risk. Using them right requires proper equipment, sizing, testing, etc... And getting people properly fit, etc was not something that was remotely practical for the general public. That's not to mention the materials used... properly protecting masks have to be made of high-quality and consistent fibers.
The current recommendations for wearing masks is not to protect the wearer of the mask. It is to protect other people. If you take it as a given that there is widespread asymptomatic cases of the virus, then you don't know if you have it or not. So wearing a mask is to protect other people from you. If you are wearing a mask, any virus that you happen to shed will be trapped as you exhale, or at least not be able to travel very far.
Unfortunately, any help that wearing a mask would offer to the wearer is often countered by the false sense of security that they bring. There are many people in masks that think they are protected so they can ignore keeping their distance from others. This is 100% wrong.
The best way to avoid germs from other people is to distance yourself from other people.
> Unfortunately, any help that wearing a mask would offer to the wearer is often countered by the false sense of security that they bring
Today's cars are extremely safe. Are you saying that they actually increase accidents because it gives people false sense of security? Should we remove some of the protections, for example the seat belt, because that would make people drive more carefully?
Tesla autopilot crashes are a closer analogy. A seatbelt is (generally) not an improperly used piece of safety equipment, it generates actual security.
> Touching one's mask is infinitely better than the alternative of touching one's face,
No, because the outside of the mask is contaminated and now your fingers are contaminated.
> and in the case of a non-symptomatic individual wearing a mask to reduce outbound infectious particles has no bearing at all.
No, because the outside of the mask is contaminated because those masks are not impermeable and the virus does penetrate it, and so now that persons fingers are contaminated and they contaminate other surfaces.
> The whole 'masks are too hard to use'
So far every single video I've seen of people who aren't HCPs wearing PPE has shown them make mistakes that lead to contamination.
"Wash your hands with soap and water for at least 20 seconds; don't touch your face" is much simpler than the protocols for donning and doffing gloves and mask.
> No, because the outside of the mask is contaminated and now your fingers are contaminated.
My understanding is that that's a misunderstanding (one that I was under as well).
For people who aren't sick, the worry is that your hands get contaminated (much more common, from surface contact), and then you touch your mask and transfer to the mask, and eventually it works its way in since these aren't N95s.
i.e. it ends up being the same as hand-mouth contact, but people think the mask is keeping them safe from that.
You inadvertently touch your face way more often when wearing a mask, that much is pretty obvious. You also are more likely to be more confident about your safety and behave in a slightly more risky way. Kind of like how cars drive closer to bikers with helmets than bikers without them.
When I am out and about, I assume that my fingers are contaminated. When I get to my car, I always do a cleanup down with an alchohol wipe and when I get home, do the ABC wash of my hands and face.
Still, wearing the mask is a constant reminder not to touch my face. some people will still ignore that reminder but not everyone is going to follow the rules 100%.
I commented on exactly this on HN a few days ago - when I venture out these days, I notice some people wearing masks, and just in the short time I see them, pretty much every one has adjusted/fiddled with their mask.
The masks I've seen are of varying types, but I guess most are of the 3M DIY/building variety (that is, masks designed to be worn while doing building work).
Maybe the government should get experts to decide the rules that other people should follow, and we should be taxed to fund these experts and their plans. That's worked so well.
I'm not sure I understand this argument. Are you speaking of sick people coming into the hospital during this pandemic or overall? Because I can ensure you, many hospitalizations are not due to a lack of PPE. Broken hips are not caused by a lack of PPE; myocardial infractions are not caused by a lack of wearing gloves; nor is a person falling into a diabetic comma caused by not wearing PPE.
But, if you're talking about during this pandemic, it was inherently clear that there was a lack of supplies to begin with and panic buying/hoarding would not help the situation. Now don't get me wrong, I am not condoning the actions of any government--I feel as if they did drop the ball--but there was a dire need of any available PPE to be given priority to first responders and frontline healthcare workers. When you're physician gets ill and eventually passes, that PT load is now given to another physician who is putting their life on the life. We need to protect those on the frontlines who are protecting us or else there will be nobody left.
People are making their own masks. There is no shortage of DIY masks. They have always been able to do that but, medical people and government leaders waited months in the USA to tell them to do that. Other countries already proved that wearing masks all the time helped protect you.
Medical people are telling the public not to wear gloves. The reasons they give and examples are detached from reality. There is a video going around on Facebook where a nurse acts like paint accurately represents cross-contamination. No consideration for material properties or other types of gloves.
This. If you change your gloves whenever you would normally wash your hands, then I fail to see why cross-contamination risk would be any higher with gloves.
People were told face masks don't work by the officials. This actively harmful lie was propagated since they wanted to save the PPE for health care workers. The problem with this approach is that one asymptotic/mild cashier can undo the work of a thousand health care workers.
At some point, I want to leave my house. Like, maybe in June?
A face shield sounds like a prudent way to reduce one’s risk while also being able to interact with others. Why not let citizens buy them after shortages end?
Of course I put on a mask, and I rarely leave the house. I was not aware they were not helpful when generally interacting with others - obviously then I wouldn’t want to wear one.
Over 1000 people in America are dying every day of this disease. This thing costs probably $2 and likely provides significant protection.
About 100 people in America die per day from motor vehicle accidents. Next I suppose you're going to tell me that the extra $50 it costs to install a seatbelt in my car is a waste of materials, time, and money too, right?
Face shields are to protect against body fluid splatter during invasive bodily procedures and while closely treating patients with explosive coughing fits. Even doctors in hospitals treating Covid-19 patients don't wear them outside those types of circumstances. There is no need for the general public to wear them. It's not like fitting your car with a seat belt, it's like fitting it with an ejector seat.
So your argument is that the risk to the average American is low from COVID? Why do we have 300,000 cases then? Why are 1000 people dying a day? That's already 0.1% of the population, and most of them in the past week!
The risk is very high, my wife is a nurse here in the UK and is infected. Fortunately she has light symptoms and a light cough. When I am with her we both wear a face mask, but there is no need for a shield because I’m not intubating her her or at risk of heavy splatter from close range explosive coughing. Again, even doctors in hospitals only wear face shields under specific circumstances, which are situations the general public are not likely to find themselves in. That’s why you don’t even see doctors and nurses wearing face shields in public or taking them home. Outside those specific circumstances they don’t need them, and we don’t need them.
I would humbly suggest that doctors very rarely deal with diseases this dangerous (infectiousness + lethality) and that more extreme protection is warranted. As you well know, it is difficult to not catch this thing.
I would much rather overdo my PPE than underdo it. Overdoing it just costs me a little time, underdoing it costs lives and injury.
If you want to see what it takes to have a hospital where no one gets infected, this is instructive. https://youtu.be/9HsGqQCLzLU
You’re not listening to what he said. He argued no such thing. You however seem content to deprive doctors and nurses of important tools and compromise their safety and patient safety so you can selfishly take something that provides zero protection to you.
Lack of testing and a laggard&lackluster response by authorities. USA will be one of the hardest hit countries in the world. There's still no stay-at-home order. Trump wants to reduce what little is being done after Easter. That's going to make the situation considerably worse.
Plenty of states have stay at home orders. Mine does. It isn’t clear to me the federal government has the authority to issue that kind of order, short of martial law. The US government isn’t identical to many other countries. States are like quasi-countries, legally, authority-wise, and culturally.
All true, but even with stay at home orders, not everyone stays home. Some people are essential workers and have to go to work. Other people go out for exercise, grocery shopping, etc. If those people have protective equipment available it is truly senseless to not wear it given the extreme danger.
Appropriate equipment yes, absolutely. But even doctors and nurses do not wear face shields routinely around hospitals. They are worn when performing particular procedures and circumstances that don’t apply to most situations even in hospitals.
Because they’re dying doesn’t mean shields will help. I think the medically inclined people in this discussion are making reasoned arguments. You however are just appealing to hysteria.
I can imagine so many other more likely reasons for those deaths than face shield usage.
Face shields aren’t protective wear in public. Taking them away from doctors and nurses however does increase mortality for them and patients in general.
These face shields are intended as an alternative to eye protection that is in short supply. They do nothing for respiratory protection. Infection via the eyes is primarily a concern for people interacting closely with contagious patients (i.e. healthcare workers).
To answer your seemingly underlying question: no, if Apple gave you a face shield it doesn't mean you get to go outside.
If no one is going outside, how are there any new cases? Lots of people are "essential workers", they go to the grocery store, the pharmacy, etc.
Yes, HCW exposure is much greater than the average person, but your argument is essentially: Since you aren't driving in a Formula 1 race where the risk of crashing is higher, there's no need to wear a seatbelt.
When we're seeing hundreds of deaths per year from COVID, I'll agree with you, but currently, HCW or no, COVID is one of the biggest threats to your life, and you'd be an idiot to go outside without the best protection you can get your hands on.
They don’t provide the general public any significant protection. It’s basically the same as not wearing one, except you’re condemning health professionals to increased risk, exposure, and possible death.
If time was of the essence for car production and we needed to decide if ambulances or regular cars get seatbelts first, then yes, we'd give them to ambulances.
I'm not suggesting that priority should not be given to HCWs or other high risk people like grocery store employees, but at $2 each, this is something everyone should be wearing as soon as we have enough of 'em.
That this article was written shows clearly that we don’t have enough of them and that any non-medical professional buying them is only contributing to the population of ill and the dead.
I think it's more that these would be a pretty involved overstep for regular people to be walking around in. Social distancing + hand washing + a homemade cloth mask is sufficient for regular people. For the same reasons that regular people don't need/shouldn't be wearing N95 masks everywhere, nor should these.
If the argument is that civilians shouldn't wear N95 masks outside, but rather donate them to people who need them even more, fine.
However, if the argument is that you shouldn't wear a $1 mask, which provides substantial protection against COVID, because it's not necessary, I would refer you again to the 1000 people that died yesterday that didn't wear an N95 mask. The amount of mental gymnastics you have to do to hold this belief is frankly astonishing.
There’s no mental gymnastics happening. You’re just ignoring what medical workers are saying and assuming your intuition is infallible. It’s easy to understand why it’s dangerous to deprive those workers of shields to benefit to yourself. And manufacturing cost is not the same as availability. We don’t have instantaneous infinite supplies of these.
If your assertion is "They wouldn't have died if they'd worn an N95 mask", I would refer you to basically any literature about what the point of wearing the masks are.
Your overwhelming condescension also make this conversation much harder than it needs to be. I would consider taking a walk and trying to relax.
Wearing an N95 mask reduces your chance of contracting SARS by 91%.
I apologize if my frustration comes through here, but the data is very clear and people are dying in the thousands because they're not protecting themselves.
It feels as though arguments will be received with claims of "mental gymnastics", so I will just point out the differences in use and function between a face shield and an N95 mask. You're free to try and purchase a face shield if you'd like.
Eh. That poster believes they've "figured it out", and those that've died just "didn't figure it out." Reasoning won't work, and unfortunately they're able to do whatever they want. I hope Apple has aggressively limited how much PPE they'll waste on civilians.
Your question was about the effectiveness of N95 masks. Hopefully I've resolved that for you. As for the effectiveness of face shields, I don't have data on that, I just said it was likely to be effective, since it blocks larger droplets from hitting your face or being inhaled.
There's no luck involved, I purchased a face shield almost two months ago, although I usually just wear mask+goggles, gloves if necessary when I need to go out. The face shield is for if one of our family members gets sick and we need to care for each other. Then it will be mask+goggles+gloves+gown+face shield.
Speculation doesn’t make you right. “Likely to” counts for not much.
It’s sad you made that purchase. I wonder if that deprived a doctor or nurse of one. If they died, you’ve essentially condemned them to that. Is your own selfish neurosis worth that?
My question was not about the effectiveness of N95 masks in a vacuum, it was correcting your assertion that the people that have died in the hospital, did so because they didn't wear N95 masks. It is possible to wear an N95 mask incorrectly, or to contaminate yourself during the putting on/taking off process. The idea that N95 masks inherently make you immune to exposure is ridiculous. The people that died in the hospital could've very well worn N95 masks and still been exposed.
I also believe you're more naive than I originally thought. I think you need luck now more than ever.
I think it's pretty simple. If you don't get the virus, you don't go to the hospital or die in the hospital. If you wear an N95 mask, according to the best data available, you have a 91% smaller chance of catching the virus.
Yes, it's possible to make mistakes donning and duffing. However, that same meta-analysis also showed a large benefit for community use of masks, so actual use, not perfect use. To the extent that there is a problem with improper use, we should be teaching people how to use them instead of telling people not to wear them.
I never said wearing a mask made you immune. Seatbelts don't eliminate your risk either, but at this point only very backwards people drive a car without one.
BTW, as of today, COVID is the leading cause of death in America.
They linked a study and then cherry picked some data from it. IIRC it was a controlled study of ~20 people, and the actual reduction % was "50-90% reduction" where every person ALSO washed their hands a minimum of 10 times per day.
I would also assert that they probably trained each participant on how to use the masks effectively, whereas I suspect OP (and most of the N95 mask hoarders) would contaminate them to the point of being useless.
edit Ah, you responded in a different place saying basically what I just said wrt contamination. Good on you.
We also know that "doffing" (taking off) the PPE is difficult, and that many healthcare professionals are infected when they take it off. I don't think most members of the public can comply with the complicated donning and doffing protocols.
More importantly, the imprints and bruises are from full-mask respirators and goggles (and one FPP3 mask), not N95 masks. Have you ever worn one (and been fitted for one)? I have, when I worked as an EMT years ago. I also have worn one N99 or N95 mask for years when cleaning out my guinea pig cages. It's not that bad.
In terms of doffing the masks, it's pretty straight-forward: To remove the mask: remove it from behind (do not touch the front of mask); discard immediately in a closed bin; clean hands with alcohol-based hand rub or soap and water (via WHO).
I'm not sure what's driving your passionate anti-mask campaign (N95 and otherwise), but I urge you to look into what doctors and public health experts have started recommending after considering the evidence and what we know about how this infection is spreading:
Absolutely stay home if you can. It's the most effective way to avoid spreading or contracting Covid-19. But wear a mask if/when you must go out (to grocery store, drugstore, essential job, etc).
As we were told during high school biology: cardiovascular muscle contains vast amounts of mitochondria as compared to other muscle types. Mitochondria are good. Therefore, more and stronger mitochondria = more efficient working muscle tissue.
One of my favorite professors holds a PhD in kinesiology (exercise physiology concentration) and wrote his dissertation on the mitochondria. As he stated many times in class: if you want to have a superhuman composition, acquire more mitochondria. he was always willing to bet his kids entire college tuition funds if you could show him a pill that would produce more mitochondria.
> Activation of Rev-ErbA-α by SR9009 in mice increases exercise capacity by increasing mitochondria counts in skeletal muscle.
> Some companies are selling SR9009 online for human use as a 'research chemical'.
> "The drug [alters] the circadian rhythm (in mice) and we would need to assume in humans – and we don't know if it is beneficial or detrimental at this point."
---
It has "several issues that make it unsuitable for human use".
> Firstly, it has no oral bioavailability. I know the company selling this is indicating taking it orally is ok – but it doesn't even get into the blood.
> SR9009 has some functional groups that are known to have potential toxicology liabilities and it would never be developed as a drug.
> So bottom line – I would never recommend using this compound at this point. That being said – we are still working on improved compounds with one of the potential uses being sarcopenia – loss of muscle and strength due to aging.
Well, it definitely is a meme as defined by Dawkins[0]. In general, I would say that analogies and metaphors like this one have a huge impact on normal science, and are one of the main things that change during a paradigm shift. I recall a great example in how 150 years ago people thought of the body's physiology as analogous to a steam engine with downstream effects due to pressure building up, contrasted to how in today's computer age, we tend to think of physiology in terms of signal processing.
I agree, the imagery that we use in metaphor (in speech, visually, or in conception) influences how we think about things - and a popular analogy like that about the mitochondria is certainly a meme, a "cultural information transfer".
As you pointed out, a fairly recent meme is "the brain is the computer of the body", and maybe "the Internet is the brain of humanity".
The cells would consume more energy, so you'd need more food, so in conditions of food scarcity (i.e. 99% of our [pre]history) you would be at a severe disadvantage as your tribe would starve to death in conditions when more efficient homo sapiens would still survive.
There are other cell types that have a strongly increased amount of mitochondria like brown adipose tissue. They also don't have a "need" to perform some work constantly.
As with any cell function how much work mitochondria perform is highly regulated. Just because you have a lot of them doesn't mean you can't turn their function down.
Nadia Commenci was recruited as a gymnast at age five because she was too active and breaking the furniture at home. She made the first ever perfect 10 score in the Olympics. They didn't have a way to display it. It got displayed as 1.00 because they only had three spaces on the sign.
Her best friend became a professional ballerina.
I have heard that Chuck Norris does two workouts a day and if he skips one, he makes everyone around him crazy. If he does two per day, he's calm, cool and collected and fine to be around. If he doesn't, welp, he can't sit still and he can't control his mouth and he bounces off the walls and everyone can't stand him.
I also talked about the addiction process and mitochondrial function in a different comment.
> I have heard that Chuck Norris does two workouts a day and if he skips one, he makes everyone around him crazy. If he does two per day, he's calm, cool and collected and fine to be around. If he doesn't, welp, he can't sit still and he can't control his mouth and he bounces off the walls and everyone can't stand him.
this is a common theme among people who do lot's of sports. I did plenty of marathons, trail competitions in my time and a day without exercise felt like absolute agony mentally. There is probably also a psychological effect from missing the routine. Most sports addicts I know (including and especially body builders) have the problem of not giving their body enough recovery time between workouts causing them to actually perform less well, etc
I have a son that I put in gymnastics when he was a child. One of his teachers basically told us "Put him on Ritalin" because he never sat still in class. ADHD had already been ruled out, so this "Let's skip diagnostics and go straight to just drugging your kid for my convenience" attitude really pissed off my husband.
If he was exhausted enough, he occasionally sat still. So he was in gymnastics for a time and, when he was younger, I just made sure to take him to the park and stuff a lot so he could run around some every single day. Otherwise, there was no hope he would actually sleep.
> this is a common theme among people who do lot's of sports. I did plenty of marathons, trail competitions in my time and a day without exercise felt like absolute agony mentally.
And then along comes coronavirus, and the privation for exercise addicts while under quarantine is so much less than what many are experiencing, but it's real—and no-one takes "it's hard not to exercise" seriously.
Top endurance athletes do specifically targeted workouts which significantly increase their skeletal muscle mitochondria density. They don't appear to have trouble resting; rather the opposite.
Endurance athletes do not routinely exhaust themselves during workouts. Instead they work out to build mitochondria (among other goals). Hence the popularity of polarized training programs. Exhaustion impairs proper rest and recovery. Your suggestion is not consistent with what we see happening in humans.
They don't remain endurance athletes by skipping workouts for months on end. I've seen articles where some body builder got the flu, couldn't workout for a week or so and lost significant amounts of muscle mass, like 25 pounds.
You develop capacity like that, you use it or lose it.
And maybe I'm not making my point very well, but everything I've seen in life suggests such people do have a real need to workout regularly. It's not a "nice to have" for them. It's a "must have."
There was even a woman who was eventually diagnosed with a genetic disorder whose disorder had long been de facto managed by her very active lifestyle.
But I'm going to step away from this discussion. It's starting to look like a pointless pissing contest and that's not really my cup of tea.
Losing “water weight” is a thing. Boxers do it as part of their weight management before their weigh-ins. When I am well-hydrated I lose ~1.5 lbs of water weight just by sleeping (by weighing myself before bed and right when I wake up). If I take a piss it’s an even 2. And we lose a lot of body fluids when we have the flu.
That wouldn’t account for all 25lbs (which is a significant sum to be losing in a week — is that even factual,? Did this guy weigh 350 lbs lean?), but it could account for a good amount of it over the span of two weeks if he was really sick and also not eating well due to lack of appetite, diarrhea, sore throat, etc. How quickly did he get his weight back? Did he lose any significant amount of strength?
The flu is not the same as being out of the gym for a week. Although we do know that you will begin to lose incrementally more and more muscle mass the longer you’ve been out of the gym, being out of the gym for one week shouldn’t lead a bodybuilder to lose 25 lbs, and sometimes it’s even part of good training strategy to take a one week break from the gym to let the nervous system recover, which gets taxed just like the muscles do.
Src: I studied Biological Science at university
Also, during my histology course when we covered different muscle types, we discussed the topic of fatigue in cardiac tissue, but I remember being left with a feeling that we didn’t really know the underlying physiology yet (this would have been nearly a decade ago) but the main arguments were that cardiac muscle is not the same as skeletal muscle, whose differences can be seen under a microscope, and that the heart has enough time to recover when it’s not contracting.
Here’s a similar question — does the esophagus ever get tired? How about the diaphragm? Do you ever get tired of breathing?
I really don't remember the details and the original article may not have listed weight loss. It may have listed inches around his biceps lost.
I just remember it being hyped a bit concerning "yeah, he looks amazing -- but you can't take a break at all because when he had the flu, he saw crazy declines in a short period of time." I want to say a week, but that could be wrong.
I'm seriously bad with remembering names, titles, etc.
I also remember a friend who took up weight training after giving birth. She said she lost four inches around her waistline and only lost four pounds because muscle mass is generally heavier than other tissues.
I've had similar conversations with other women who were trying to lose weight or otherwise work on their physique. Some are downright disappointed by such results because they are looking for a specific number on the scale.
Sort of tangential: I knew a woman who quit smoking. Smoking suppresses the appetite and meets oral needs. People who quit often take up snacking as a substitute and their weight shoots up.
She said she would weigh herself and cry and her husband would basically talk her out of taking up smoking again because she was so upset at the weight gain.
Anyway, my mind organizes info its own way and I'm not always happy about it and it sometimes gets me into all kinds of social hot water because it sounds like crazy talk to other people. So this is probably not going to get better from here.
It isn't physically possible to lose 25 pounds of lean muscle mass in a few weeks. That's off by an order of magnitude, check the energy and mass balance calculation.
But frequent exercise is certainly a "miracle drug" in that it effectively prevents or treats a host of different medical and psychological conditions.
Edit: I will add that I am also, no doubt, basing it off of background knowledge about cell function. For example, mitochondria change and develop greater capacity to process X if you consume a lot of it, which is part of the addiction process and part of why withdrawal is a thing. If you consume a lot of, say, alcohol, you need to ramp down gradually so that the body can make changes at the cellular level to adjust to the lesser amount of alcohol and this is part of why cold turkey is so very hard and it is generally recommended that you taper off.
I used to ask smart people with PhDs and the like a lot of questions about cell function and read what I could get my hands on that could be followed by a lay person because I have a genetic disorder that impacts cell function.
Non-repetitive weight lifting wouldn't be a good example, but neither is anything in 10s of km.
Mitochondria produce ATP as energy. You can't store much¹ ATP, therefore mitochondria must be capable of producing ATP at your near peak output (say 10s average).
I'd look at anything with high >10s peak power (probably a bonus if it's aerobic). Many bodybuilding exercises would qualify.
¹ Lactic acid is a byproduct of ATP production, therefore ATP supplies surely last less, than what it takes to start producing lots of lactic acid.
Aren't mitochondria captive cells from early evolutionary times?
I googled and from nature.com
"Mitochondria and chloroplasts likely evolved from engulfed prokaryotes that once lived as independent organisms. At some point, a eukaryotic cell engulfed an aerobic prokaryote, which then formed an endosymbiotic relationship with the host eukaryote, gradually developing into a mitochondrion."
> If the heart is a muscle, why doesn't it get tired?
Because it's illogical to assume muscles fatigue. They physically don't get to the point where they can no longer operate -- under normal everyday use and exercise.
What does happen, that may seem like fatigue, is a gradual shifting of fuel sources by muscle cells depending on exertion levels.
Suffice to say, it goes like this:
- First: Creatine Phosphate is the first energy source in your muscles, the most powerful one, and the least plentiful. It's the first to go during exercise and is partly why you focus on 1-5 reps for strength-focused lifting (that's roughly how long it takes to get used up)
- Second: Glycogen in your muscles and liver. This is fairly plentiful, fairly powerful, and rapidly mobilizeable. After your creatine phosphate stores are emptied, glycogen takes over. This is still a very powerful fuel source, but its metabolism creates a negative feedback loop on itself. You can only sustain moderate exertion (see: sprinting or 8-15 reps moderate weight) for around 60-90 seconds, before glycogen is no longer easily accessible (note: accessible, not depleted. It's almost impossible to deplete in a single workout)
- Finally: Fat. Once you've exhausted glycogen, your body turns to fatty acid oxidation. This is the least powerful but most plentiful. In normal exercise you use a mix of fat and glycogen depending on how hard you exert yourself. Harder: more glycogen. Easier: more fat. If you want to know how it feels like to run on only fat: do a marathon -- then hit the wall. What you experience is literally the complete depletion of glycogen, and a transition into "low-power" mode as your body starts running on the only fuel source it has left: fat. You have months of this fuel source on your body, you won't run out. You can keep walking for days without having eaten anything or slept, but you won't be able to run at any pace that resembles a jog. I know, because I have.
What's the point of all this? It's to illustrate that muscle "exhaustion" is a misnomer. Muscle exhaustion is, in reality, a depletion of power-generating fuels leading to a state of minimal exertion.
Coincidentally, that's the mode the heart operates in 24/7.
Coincidentally, the heart has an asinine amount of mitochondria to fuel non-stop fatty acid oxidation.
The heart doesn't fatigue because it's not physically possible. It doesn't need creatine phosphate or glycogen (very very little) to pump blood. It's not a strenuous task.
An aside: if you had as much mitochondria in all your cells, as you do in your heart's, you would waste away.
Some anecdata but, I suffered from very bad muscle injuries from one summer in 2014. I skateboarded hard for two days in a row. Ran 3-ish miles on both days. Two days later I was exhausted but took two ibuprofen and I went to a beach with friends anyway. Where I skated hard at a park for a few hours, then swam, then ran. A day or so later, after not getting the best sleep, on an hour drive home, I pull both quads. The day after I had to call out for a week. I was exhausted and my obliques, core, quads, and arms were beyond sore. I laid around for most of the week.
Your muscles may not get "exhausted" but it seems like there must be some breakdown in the cells that outpace recovery at some point.
When they work, muscles break fibers. The more intensely you work out, the more they break. So you have to rest for them to be rebuilt (and more fit to the exercise), otherwise at some point they give in. The more frequently you train, the more they can withstand.
That seems unlikely given that if he had rhabdo he’d have felt bad enough to need to go to hospital. 20% death rate due to kidney failure is not to be sneezed at.
You can't really exert yourself to the point of a heart attack unless there is some other pre-existing condition like a congenital heart defect, arterial blockage, history of cocaine use, etc.
Then I guess the obvious question a non-physiologist would ask is, why don't all our muscles already have vast amounts of mitochondria? If it's that beneficial with no major downsides then surely evolution would have stumbled on that configuration already?
Because the trade-offs are not optimal for most people. Might require huge caloric budgets not available (until now). At present, energy efficiency is actually detrimental to reproduction for most people in first world countries, so it's conceivable if we wait another million years or something, our muscles might have a lot. Assuming not getting tired leads to reproductive success, of course.
For a vast amount of human history food has been much harder to obtain and less calorie-dense than it is today, so evolution has optimized for energy efficiency rather than raw power.
Significantly, and a large part of the reason why is energy efficiency. Humans have large brains that take a lot of calories to sustain, and because of their large brains didn't have nearly as strong evolutionary pressure to maintain musculature.
Probably the wrong way to look at it. They can exert greater force for shorter periods but the great apes have far worse endurance than humans. A chimp is about a third stronger than a human of equivalent weight but we can run marathons and they can’t. We have a higher proportion of slow twitch muscle fibres compared to fast twitch than the great apes.
Think of evolution as Uncle Fester from the Addams Family.
You never know quite what you'll find him working on, but every now and again, he'll have just the thing for the job.
But by and large, it's most likely something completely insane. Evolution has no intent. No direction. It's more a descriptive statement of an ongoing process than a end to which some force is constantly seeking.
not only energy expensive but free radicals do genetic damage, and a this requires the second budget for a set of enzymes to counteract the damages and scrub out FR's
Muscle cells don't replicate past early childhood development, they just get bigger and add more nuclei. So muscle cancers are extremely rare compared to cancers of other tissues.
each nucleus contains a full genomic content.
muscles are more of a "myosynsynctium" than a group of cells.
there are cohorts of cells that are more prone to becoming cancer due to thier developmental origins and the complement of developmental mechanisms that can be reactivated.
things such as cell adhesion, and cell migration through tissue dermal cells are good at this as they do these things over the course of development.
muscles are built where they will live so these features are inhibited somewhat more completely and harder to "switch on or off"
Neat, but why don't all the cells in our body do that? What's the trade-off that goes the other way for cells most likely to get cancer (prostate, breast, lungs, lymph nodes)?
As others pointed out, an increased output would not be sustainable long term within the normal body. The physiology behind action potential[1] and refractory period[2] explains how they compliment each other to make sure our system function properly and effective.
Not unless having vast amounts of mitochondria is a competitive survival/reproductive advantage favoring natural selection of individuals in their environments
He would have lost his sons college thition then. Mitochondrial _inhibition_ is actually more correlated with longevity than the other way around.
If more mitochondria meant more efficient working muscle tissue, then that's what we would have evolved, there's always a compromise. Are you sure you can keep the same power output for a given mass and volume of muscle if you keep increasing mitochondrial numbers? Even the reddit answer clearly says that the heart muscle is rate limited by oxygenation (they have more mitochondria but are also highly vascularized to power the mitochondria). More mitochondria===more power doesn't mean it's better for us, physiology is rarely that simple.
Specifically it is due to reproductive defects in mitochondrial dna as one ages. Anti-aging researcher Aubrey de Gray has a talk on this specific issue:
But evolution didn't decide on the structure and behavior of our throw-away-cup bodies in order to make our puny minds sitting on top our puny brains happy.
For better or for worse, in humans (we are not turtles, for example, they have their own success strategy), AVERAGE 2nd generation reproductive success is the measure of our existence. The collection of strategies to maximize that are different for human men and human women. But aligned. On average. 2nd-generation reproductive success is our "purpose" in a universe made mostly out of hydrogen. Nothing more - nothing less.
I've seen videos of NYPD going in and telling people in restaurants to clear out (from days ago). I wouldn't be surprised to see NYPD telling people to clear out for this too.
More broadly, if you live in NYC and know the NYPD, then of course they're going to respond in this manner when such orders come out. When they have authority, they use it.
If someone wants to exercise their freedoms and accept responsibility for harm they cause to themselves, I don't have a problem with that. I do however have a problem with someone's exercise of their freedoms causing physical harm to me without my consent. In the same way that it's not acceptable to get lit and then drive a car because it creates a risk to other people, people should shut up and stay inside when told to do so in this context as they risk getting sick or being sick and spreading the disease to others, potentially killing them.
That's how it should work. Excellent example. Automobile deaths account for over 3000 deaths per day, far in excess of what covid19 has or will do.
Given that information, it seems that you would recommend people "shut up and stay inside" due to the "risk to other people". This is not rational.
Giving up everyone's freedom and accepting simple authoritarian solutions a few vocal people want is not a good approach. Punishing perfectly healthy people by threat of imprisonment as a result of the absence of planning by the nation's healthcare and government is not a reasonable response.
That 3000+ per day is for the entire globe. And horrifyingly, there’s a chance the US alone will surpass that for some period in the coming weeks. Italy recorded 600+ today, and we’re much bigger. Plus we are way behind on locking down.
> Downside is that transferring into competitive top ranked programs is very difficult.
What type of “top ranked” program are we talking about here? If parent is trying to get into MIT after a long educational hiatus, then, ok, maybe it’d be a bit difficult. But if they’re hoping to obtain an EE or CS degree (for example), these programs—in the states—are usually accredited and if their engineering program is not accredited, you shouldn’t even entertain the idea of entering that program.
There seems to be this constant myth that comes up when talking about higher education and that is a top ranking = better. Don’t get me wrong, a social science education from Yale or Brown will differ greatly then one at a state school but that is a given. Same goes for the select engineering programs or CS—think Cal, Georgia, MIT, etc.—but something like engineering is a program that has to follow strict course requirements so your end goal is practically the same no matter what your alma mater is.
Public schools are what I'm talking about - the ones people would actually transfer to. (UCB, UCLA, UW (where I went), UT Austin - all top ranked CS program schools) Private is much worse. You'll probably never get into a top private school unless you're transferring from another top tier institution - most people I saw transferring into such schools were already from other top tier schools. Stanford, for instance, accepted 27 transfer students last year. 27 - that's it. Same story for many other prestigious colleges.
The point of going to a top program isn't that it's a better program academically (maybe it is - maybe it isn't). It's about the resume and other things the university offers. Some of the schools help place you in co-op programs, have catered career fairs, and much more. They can set you far apart from other "lower tier" schools and make you stand out in the overwhelming crowd of new grads. It's mostly about signalling more than anything.
Stanford's undergraduate enrollment is 7,087. Very very few if any of those 27 transfers were from JCs. Berkeley's undergraduate enrollment is 30,853. About 4,617 JC transfer students were offered admission.
For California in specific, there are special legal privileges for transfer applications from community colleges to the UC system. That's what you're supposed to do as a community college student, so e.g. it's easier to transfer into a UC from a community college than from a CSU, even though the CSU students are, by design, superior to the community college students.
I'm curious where you get your statistics from? Do they break down the transfer students' details, ie, how many of them are US students and how many are from China? The competition against rich Chinese students for getting accepted into Cal has gotten more and more fierce the past 20 years.
UW being University of Washington? I transferred into UW CSE from N Seattle Community College as did many others! We had maybe 3.7+ GPAs in community college and intro courses overall.
Private like ivy leagues didn’t make sense for me then because tuition assistance was so poor. Unless you’re super highly ranked and can get a ton of merit based scholarships that was a bad idea anyway.
However, it’s perfectly reasonable to work hard in undergrad as a researcher and student then make your way into the top tier. James Mickens is a great example of this path. This is obviously not for everyone but neither are private world acclaimed universities.
> Private like ivy leagues didn’t make sense for me then because tuition assistance was so poor. Unless you’re super highly ranked and can get a ton of merit based scholarships that was a bad idea anyway.
Another option (depending on the school) is low to no tuition if coming from a lower income family. I want to say it’s Stanford but i may be wrong, that offers free tuition to eligible students whose family income was less than something like $50,000/yr. So there are ways for poor students to get a great ivy league education but like you said, you must also have extremely high rankings in your class to attempt that route.
Depends on the year. I mean, they take like over 5x the students now than they did when I was there. For the time I was going, they weren't accepting transfer students like myself with anything shy of a 3.9. I think that was the lowest I saw for accepted on the stats website.
I had a 4.0 before I moved up to Seattle. I thought it was going to be a done deal but then I got some bad professors and it screwed me over. Quite unfortunate.
I don't think people need to get into top private schools. It's just a matter of how hard you want to work after college because you won't have had the same footing as those other folks.
Sometimes I wonder if signaliing is the real 'value' they offer that people seem to want to work for, the problem isn't as much the education as it is.. everything else.
knowledge is knowledge, no matter where you obtained it. However, the connections you make during college is sometimes quite important, as they are the windows of opportunity that aren't available to the non-connected. E.g., if you have a friend in the same class, then they are more likely to refer you to their company if you are in need of a job (later in life). Or if they are already rich and are investors, you are more likely to be considered to be confounders or business partners.
If you want to run an already very large business your best bet is to go in to management consulting. In that case what you study is less important than getting top grades at a top school and interviewing like a champ.
If you want to run a business that isn't but has the potential to maybe be very large then easiest way to do that is to build your own and CS has a very low bar for entrepreneurial activity.
If you just want to run any business then no degree necessary. Just work in food service and treat it like a career. Maybe do a bookkeeping course. You'll get to manage a restaurant eventually.
You should check out the book The Case Against Education if you want to pull on that thread a little more with signaling. It's a compelling book for me.
Well, yes, of course it is. If someone graduated from Oxford or Harvard then the reputation will follow them for the rest of their lives. It’s bizarre really but it’s also so normal that no one ever stops to question it. Same with some companies, e.g Google, they are 100,000 people now, very far from an elite, but work there even for a few months and you will be an ex-Googler for the rest of your life.
Maybe Netflix? The others are just on a level with IBM or HP or MS or whoever now. Big tech companies staffed with average engineers. They are coasting on reputations earned when they were just a few hundred of the best engineers.
Don't know. But you can get better opportunities everywhere with G on your resume over Amazon. Amazon also pays way less and has worse perks in everyway. Google was known to be a great place to work. That legend carries on amongst non tech people.
> and if their engineering program is not accredited, you shouldn’t even entertain the idea of entering that program
Did you know that, for example, Stanford’s CS program is not accredited?
Do you think people shouldn’t entertain the idea of going to Stanford for CS?!
> something like engineering is a program that has to follow strict course requirements
From what I know accreditation sets a super low bar because it’s all above that bar. What colleges teach varies massively. You definitely can go to a lower ranked but still accredited college and come out with massive gaps in your knowledge compared to an unaccredited program like Stanford that would push you much more.
> this constant myth that comes up when talking about higher education and that is a top ranking = better
I don’t think that any of us think that, but there are people doing the hiring that do think that. There are jobs you can get if you graduated from MIT that you can’t get if you graduated from Idaho State. Mr. Idaho State will find a job, and it will be a good job, but Mr. MIT will find a better one.
Tesla has always had body alignment issues since their first attempt, the Model S. It’s honestly quite unfortunate because these models are suppose to be a shiny example of American manual labor pushing out the new luxury model that would set Tesla up to enter the mid level market with a Model 3. Sadly, technological advances, a backlog of orders, and minimal factory space, all contributed to a decline in quality. Don’t get me wrong, these are absolutely beautiful cars, but in terms of actual construction of the vehicles, GM and Ford has nailed this to perfection with their automatic + human labor assembly lines. They’re able to produce numbers right now that Tesla can only dream about with a much higher satisfaction rate, I would think.
If Musk wants to really compete with the Big 3, he has to focus on quality all the way around and not just the ability to slap bigger batteries in and more speed through firmware updates. If you want to make a car, focus on the basics of it—the actual body, making sure my door lines up with my front fenders. Such basic cosmetic issues that are overlooked constantly on the cars coming from the Tesla factory.
The quality on the 3 is fine. I've heard so many panel gap anecdotes and "fit and finish" problem that I was a bit excessive in my inspection of my Model 3 before I took delivery (November 2018). It was fine. There are no quality problems that I've been able to ascertain. The only real kind of weird thing is the polarized glass on the roof turns a really strange but beautiful color when it gets wet.
The car drives like nothing I've ever driven, not even a higher end mercedes.
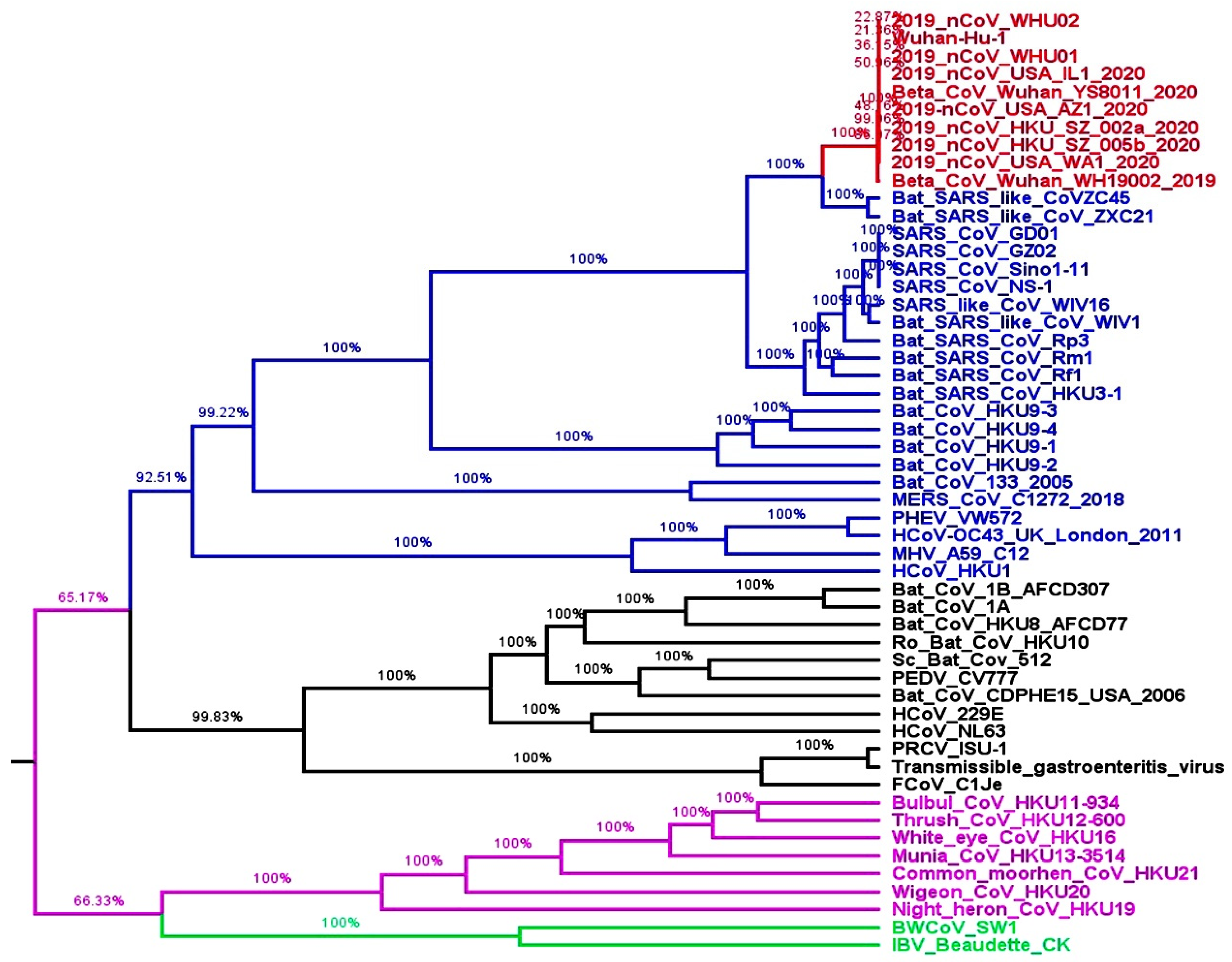{kind=link}