My 3 year old daughter was recently diagnosed Type 1. Soon after her diagnosis I discovered a heap of articles about the Open Insulin Foundation. I was even on their website 24 hours ago. However, for the life of me I can't find anything "open" about the Open Insulin Foundation.
Could someone please point me in the right direction where I can read anything with more substance than a news article quoting an interview?
EDIT: Just to clarify. We're extremely fortunate that we're in Australia. Insulin is affordable/subsidised here, my daughter's CGM (and sensors) are free, and anything else we need is heavily subsidised too. I've no intention of biohacking anything to do with my daughter's Type 1.
I'm asking the above mostly because I'm curious. Admittedly I find it a bit scary that I know so little about the manufacturing of something that is 100% vital to my daughter's survival. I'd like to know more.
Hi, I am one of the scientists working on the project.
We had a lot of discussion on the project about defensive strategies to avoid any issue, since we are dealing with a massive industry. We don't have a definitive protocol yet, so this is why it is not publish. But if you want more details, I would be happy to answer your questions.
I've seen a lot of projects like yours with the purest of goals never get past this stage because, simply, nobody makes the first move. It's almost like the attention gets in the way of publication. Either that, or there was never anything there, and it was just good PR from the beginning.
Your project is too damn important to let this happen. Please find or do whatever you have to do in order to publish what needs to be published. If that means taking a leap of faith, please, for the love of goodness, please do it.
I forgot to mention it, but there is also FDA requirement to how we disclose the protocol. Usually it is patented process, so we are looking to see how we should do it to not create issue for the FDA validation.
Other volunteer are working on this side, not me. I am a simple biochemist, those things are two complicated for me.
It is a risk, I agree. I can assure you that there is work done in the lab, and that we plan to publish it, one way or another.
I personally think that bioRxiv can be perfect to do a fast publication.
TFA blames "big pharma's stranglehold" for high insulin prices, but interestingly the cheapinsulin.org explanation [1] seems to be much more about "big insurance", with pharma companies basically forced to kow-tow if they want their products to be covered.
Their claim is that if the pharma companies lowered the cost of insulin but then refused to give rebates to insurance companies for it, the insurance companies would stop covering insulin for diabetic patients? And they're using a diagram created by a pharmaceutical trade group to explain this? I'll be honest: I'm skeptical.
It’s a pretty… lame argument. The insulin maker is saying they want to lower the price for you, but hose the insurance company.
Frankly, we should nationalize insulin production and stop people and insurance plans from going broke buying it. Imagine if Medicaid wasn’t paying usurious margins for a commodity that has been around for a century.
Unfortunately this is pretty accurate. Pharmacy Benefit Managers (PBMs) are contracted by insurers to set the formulary, in effect the list of drugs the insurer will pay for. They negotiate to lower drug costs, usually via manufacturer rebates.
Where this is perverted, is that the PBMs have complex compensation schedules wherein they receive a percentage of drug rebates. Their goal is to secure the largest rebate possible. Thus, either negotiate more effectively OR pressure manufacturers to increase list prices and give larger rebates. In practice, the latter happens most often. Insurers don't mind high list prices because they get large rebates and it encourages people to stay insured. Net prices (pharma revenue) on off-patent insulin have declined consistently since mid-2000s [0].
However, insulin is inexcusably expensive due to legacy regulation about equivalence for biologics and sticky patient preferences. Even current net prices are 2-5x too high relative to what a competitive generic market could produce.
All these complicated incentives make it hard to figure out who's responsible, so let me ask a question:
What if a manufacturer lowered the price of insulin to $10 a month and gave no rebates at all? Would insurance companies refuse to cover it and pharmacies refuse to carry it?
I think the problem is that this isn't in either of their interests. The insurers benefit from high prices because it scares people into staying insured and, IIRC, the laws limit the percentage of their profits, so a percentage of a higher number means more profit. The drug companies more obviously benefit from high prices.
Every time this stuff comes up it feels like we focus on the politics and not the people with diabetes.
If you or your kid or your friends have Type 1 and are struggling to make your insulin out of pockets please, please, please call the Eli Lily hotline and get the copay card. They've dropped the monthly cost for Humalog to $35.
Every drug company gives away their drugs for free to people who can't afford it in the US. It's sad that not enough people take advantage of patient assistance programs.
This is apologist thinking at best, intentionally misleading at worst.
You are correct that companies do have patient assistance programs. What you’re leaving out is that this applies to a small subset of people that usually have to be denied federal/state insurance, not have any other kind of insurance, and make less than 4x federal poverty level.
additionally, they rarely provide a lifelong supply. Imagine being a diabetic and novo nordisk, who makes most of the insulin types on the market, only gives you a four month supply.
Oh wait, thats exactly the terms of their patient assistance program.
There are some examples like Truvada which seem to be very open.
Gilead would reimburse any out of pocket costs.
Even still it's just a sick game to bilk insurance companies, and thus us insurance premium payers, out of more money while pretending to be looking out for consumers. The monthly cost on my really great insurance was still over $1k out of pocket, which took a bunch of paper work and over a month to get back. Poor people don't have that luxury.
Oh and now that Gilead's license has run out they have a new very expensive PrEP drug magically appear. Which they tout doesn't have as bad long term downside on your organs. The skeptic in me seems to think the timing is too perfect. if there is a safer drug throw it out asap. maybe they did, I can't know that but I have a strong distaste for Gilead in particular.
For-profit healthcare is one of the biggest moral failings of our country.
Not only that, but the people who most need the assistance are also the likeliest to have trouble jumping through all the hoops. I used to work for a nonprofit who would administer these patient assistance programs and after a while I felt like I was just getting a lower wage for being part of what was clearly mostly a service to for-profit companies.
Not only this, on top of it all - as if it's not hard enough to ask for 'handouts' - they require you to submit evidence that you don't make too much money.
Just a W-2 or a federal tax return should do - not like those poor people should care about their data or privacy or dignity or anything ~s
No, they really don't. Some don't offer much of anything. Many of those end up providing benefits for the poorest of the poor, but if you're a little above that you're out of luck. Also if you have something like Medicare you can hit certain phases in coverage where you have to pay a much larger part of the cost. Being on any government program disqualifies you from most of these discount programs, so if you're on an expensive Rx you can still be stuck paying a few hundred $$ a month-- more than many can afford.
These discount programs aren't some big secret people don't know about. I see that argument thrown out in defense of high prices but it simply isn't true. Every doctor prescribing drugs knows about them and tells their patients about them. If people are going without necessary medication because they don't know about a discount program then they are extreme outliers.
These discount programs are simply marketing & lobbying tools used to give politicians cover when they all continue to ignore meaningful healthcare reform.
Many people simply don’t know about them! I grew up poor and the amount of work that goes into finding and using some services is ridiculous. We bought a house using some assistance programs and at a couple points were speeding across the city to get paperwork in by sone deadline no one told us about (luckily we had a car!).
Not to mention that services like foodstamps can be unreliable… I’ve probably spent hours of my life holding up checkout lines because my card didn’t process…
not having money is one thing, but being poor also obliterates your time if you use various services…which in my experience is worse… you’re always tired and agitated. Someone is always messing up your paperwork, because of course civil servants are often underpaid and overworked themselves.
I had a similar upbringing. All the hours of my childhood in the local health and human services offices and WIC nutritional centers turned me off of civil servants and bureaucrats. It felt like they were always condescending and snippy, or pretending my parents' English was way harder to understand than it is, or just delighting in telling us our stuff was out of order.
Looking back they were probably just overworked and exhausted, but man.
I felt the same for a while too, but then I met someone that happened to work for child services. These are some caring and empathetic people working for peanuts and they aren’t really treated well by anyone, management and clients alike. This person in particular hated the work but didn’t want to quit for fear of letting their clients (children) down.
People blame bureaucracy, and maybe there’s some truth there, but if these people were treated half as well as many tech workers are then maybe we could actually start making progress against the stereotype of miserable experiences.
It's real easy to become a jaded clock puncher when you're a social worker on a six person team that can barely eek out three people's worth of work because three of the people are deadbeats who's only qualifications are an ability to deposit paychecks and knowing someone who was owed a favor by a politician or appointed high level bureaucrat. The one party states have it the worst because the "next guy's cronies" can't clean house without annoying people within their own network because they're all from the same party. That's assuming they're not union positions and they can actually be fired or laid off in a practical manner.
Nobody who has drive and wants to get shit done lasts very long in that environment. There are occasional pockets of "good" but they don't last because when they accomplish too much people move up and out or they get reigned in by the rest of the system.
Source: members of my household work in government providing social services.
Ah yes. The new administration's "house cleaning."
Better known by the people who actually work there as, "Shoving a bunch of people and papers around to show you're changing things, with no plan, strategy, or even background information to support a single thing."
If you think alternating parties solves the problems, you have another think coming your way!
Call me cynical but I don't think that's necessarily seen as a downside by the people in charge. It lets you have it both ways to technically offer assistance that many people find too difficult to actually get.
It means “the manufacturer realizes they won’t get the price they charge from other channels from you, so is willing to settle for the PR and tax benefits (and whatever residual cost is still charged) rather than nothing.
> I mean in many cases the product is still profitable for them at the reduced rate, but why settle?
Because for a customer who would pay nothing if their only choice was to get the drug at full price, settling for a reduced price (especially when you also get a tax deduction, and some PR benefit from advertising the discount for the needy) is more profitable than not settling.
> Every drug company gives away their drugs for free to people who can't afford it in the US
I don't believe this is universally true though. For example, patent-encumbered novel delivery mechanisms for existing (generic) drugs, like Concerta. The drug company has nothing to gain by maintaining the administrative infrastructure for patient-assistance for drugs like that.
Another example are personalised therpaies, such as immunotherapy treatments - which cost so much because (as I understand it, please correct me if I'm wrong) they require individual experts to develop the personalized antibodies and whatnot - unlike with mass-produced medication pills/tablets/capsules that have negligible marginal cost: a company isn't going to give away a $100k therapeutic drug for free because it still is going to cost them $50k+ (numbers just made up btw).
> Every drug company gives away their drugs for free to people who can't afford it in the US
No, they don’t all provide their drugs for free, but most of them offer directly or fund assistance programs that provide either free or reduced cost drugs.
It’s amazing that you’re privy to this information!
I kind of figured all of the dead diabetics in the US that I’ve read about over the years was the result of a structural problem with our healthcare system. Apparently this is maybe an issue with suboptimal Google AdSense campaigns that led to fewer diabetics knowing about the font of free insulin?
What a revelation that the manufacturers that control the pricing of this life-saving drug (and apparently all other drugs) are actually blameless in every scenario and that anybody that rations and/or dies does so to themselves due to being dumb.
I should clarify that I’ve lived with T1D folks in the US for my entire life and I’ve seen them have to choose between food/rent/car insurance/etc and insulin more times than I can count.
The comment that I’m responding to strikes me as either alarmingly uninformed about the material conditions that many, many diabetics find themselves in, naïveté based around completely believing some marketing pamphlet, or genuinely making statements in bad faith. I chose to respond in a sarcastic way in my previous comment because the nature of that statement is so incredibly outlandish and broad that it genuinely seems like a comment in bad faith.
“All pharmaceuticals are free if you just go to the website” is genuinely such a dada-esque-ly untrue statements for the majority of Americans that I can only imagine a person making that statement as a joke or a lie.
Ah, but are those assistance programs available to people on Medicare or Medicaid? I know a diabetic on Medicare so I've watched ads and lots of the ones that mention how little your copay can be seem to have a little note at the bottom of the screen "for patients on commercial insurance."
Thanks, I'll pass that along to her. I think the insulin is a new thing this year, so it's possible she's not on a Part D plan in the "insulin savings model."
> please, please, please call the Eli Lily hotline and get the copay card.
While this is a great thing, it's also necessary that you be prepared to fork over personal data - especially proof of income - and otherwise do whatever is required to prove that you are (un?)worthy enough as with any similar medical financial aid program.
Exactly, they just want to suck you dry. They don't want to let a̶ ̶p̶o̶t̶e̶n̶t̶i̶a̶l̶ ̶s̶o̶u̶r̶c̶e̶ ̶o̶f̶ ̶r̶e̶v̶e̶n̶u̶e̶ you die from lack of medicine that costs them pennies.
I believe that regardless of whether someone is at a financial disadvantage, neither business nor government should have the ability force them to surrender both dignity and personal financial information in order to receive aid.
It's hard enough to ask for help without having to lay your life bare to strangers in order to receive it.
As someone who had to create transgenic E.coli in a lab, I admire the effort. It’s hard to get it right, especially when trying to make bacteria produce stuff for you. However, it feels like a huge step backward. Imagine you couldn’t afford to buy a piece of bread. Instead, you need to grow your own grains and build a windmill first. Sounds ridiculous in 2021.
transgenic E coli is easy, not sure what you think is hard.
Insulin, though is possibly one of the most nightmarishly difficult proteins to make. It's kind of astonishing to me that Insulin was both the first protein sequenced and the first pharmaceutically relevant protein synthesized. Mother necessity, I suppose.
Genentech started making separated-chain insulin in E coli, back in the day, and that is emphatically not how it is done today. You get a whole bunch of crap because you need to keep the two chains denatured, and that results in scrambled disulfide bonds. If you try to do it in protein-folding conditions, one of the chains crashes out into plaques structurally similar to alzheimer's plaques.
You could make it as a single-chain protein, and then cleave out the middle section, except that the protease that you would use to cleave it out has another site internally!! And all of the proteases which leave a "clean end" leave a "clean end" in the wrong direction to yield a good insulin molecule.
Industrially, insulin is made (in yeast, not E coli) by going ahead and cleaving at that extra site, and then performing a reverse proteolysis to install a synthetically generated peptide, restoring the molecule. That's also why most insulin variants (e.g. humalog) have mutations in the tail end, that's the part that is "reinstalled". Note how crazy this is. Proteases are usually used to break proteins apart. Although technically all chemical reactions are indeed reversible, to force the chemical reaction in the other direction, you're fighting entropy, to put humpty dumpty back together again.
Honestly OIP's best shot is probably Michael Weiss' one-chain insulin molecule, which should have gone off-patent this year (https://patents.google.com/patent/US8192957B2/en) (15 years, right? IANAL) but for some reason got extended to 2028!!
However, the big danger with insulin analogs is that you really need to test the F out of them because insulin cross-reacts with the IGF-1 pathway and cause cell hypergrowth = cancer. I would also be very careful with home-made stuff because I would need to be convinced that the forumlation whipped up doesn't change the properties in such a way to to increase IGF-1 activation.
I advised Open Insulin on a ton of stuff in the first few months, but they took literally none of my advice on anything, and last I checked their mailing list a few years ago they were still stuck on some stuff I warned them about (e.g. insulin doesn't stain in coomassie blue -- another thing which makes insulin a pain in the ass).
I agree with the sentiment but decentralizing and downscaling production is a win for resiliency. This is a good example but others include recycling and power generation have clearer benefits
I think you are severely underestimating what it takes to produce a protein drug like insulin. Getting the bug to make it is just the first step. Then next step is purifying it. Which takes SO much water, and salts, and specialized equipment (resins, columns, high-pressure apparatus). A decentralized insulin production scheme is going to be VERY ecologically destructive.
The people plugged into the solar utility co-op on Kaua'i actually end up having a smaller carbon footprint than those generating solar power off the grid.
Those econmies of scale are simply driving up profits for an oligopoly that uses IP laws and acquisitions to extract maximum value from sick people.
We could revoke the
IP and thus force these companies to compete on price... but that hasn't happened. Thus the only solution that is making any progress is circumventing the IP and developing an open process.
It's unclear to me if the lack of competition is due to IP laws. For all I know, they've been coasting with the same production methods for 20+ years (the article mentions that insulin was relatively cheap in 2002). With such large profit margins there wouldn't be much incentive to improve anything.
I don't know the exact details and I could be wrong, but my understanding is:
There is IP around the production process (specifically the genetic strain of e-coli). Because the production process is biological, generics produced with a different process are not automatically approved by the FDA and have to undergo an expensive approval process. Thus the goal here is to devolop a process with open IP and get that process approved.
The problem is that patent system is a joke, and the description is likely broken (or incomplete) enough so that even a bunch of experts will have to experiment with the process to decrypt it.
You really need to buy out trade secrets of this particular brand.
There's nothing ridiculous about the fact that your wife enjoys baking bread.
There's a lot that's ridiculous about bread being so expensive that recreating the entire supply chain in your backyard is the only economically viable option for obtaining it.
The metaphor pretty clearly was not about critiquing baking as a hobby.
Their point was why are people being FORCED to produce a diabetes bio-hack instead of getting insulin. Neither your wife, Amish people, nor home mechanics are forced to make their own bread instead of buying it - they are all choosing to even though bread is cheap and easily available.
It’s clear from your responses that you seriously can’t handle logical disagreements to your point on online forums and choose to get offended instead.
The replying comment is right, it’s irrational & you’re filled with hubris to think that you could replicate world wide supply chains in your back yard. In no universe does growing yeast == replicating a global supply chain.
Growing wheat and grinding it out into flour isn’t something I’ve ever heard anyone take on as a hobby before. Having all that actually cost less (including time) than buying bread would be a huge achievement!
Adam Ragusea actually just did a 2 part video on growing his own bread from scratch in his backyard. Part 2 just came out a few hours ago.
Spoiler :P it definitely took way more time an effort than buying flour from the store and making bread. And the final product was a pretty poor loaf of bread because he couldn't find a way to buy the same type of wheat most farms use and had to settle for "animal feed" quality seeds.
I imagine the guy who built his own toaster from scratch probably also contemplating rebuilding the entire pipeline to produce the input to the toast. "Step one: acquire the ore. Step two: smelting iron ore..." http://www.thetoasterproject.org/page2.htm
It’s a little more complicated than that. Bread is ingested through a system optimized to absorb nutrients from outside the body.
Insulin must make it into the bloodstream intact, typically through injection. It’s also incredibly potent, a unit of insulin dried to crystalline form weighs less than 40 micrograms, so it much be administered in a sterile carrier fluid.
Lastly the penalty for overdosing is generally called insulin shock or diabetic hypoglycemia, and ‘it is rare but possible for diabetic hypoglycemia to result in brain damage or death. Indeed, an estimated 2–4% of deaths of people with type 1 diabetes mellitus have been attributed to hypoglycemia.‘ [1]
On the other hand, glucose blood levels are reasonably easily measurable and being slightly on the high side is fine, but the precision pumps (or microfluidics) to do this dosing automatically and accurately are still expensive.
Growing enough viable yeast to bake 10 loaves of bread is orders of magnitude simpler than growing, harvesting, threshing, and milling enough grain to bake 10 loaves of bread.
most times the results will be contaminated by bacteria. The knowledge of what was actually going on when you do this was only gained in the past 250 years or so (before that, yeast was known as godisgreat).
In addition to doing it the way you described (put out flour and water in a bowl and wait for it to bubble and smell nice), you can also buy a $100 microscope, collect wild yeast, clean the bactiera off, and grow mass cultures. Sometimes it pays to work at the last step of the industrial, scientific and agricultural revolutions.
Let's go back to before real agriculture. 10K years ago People harvested wild grain, processed it, managed to make yeast starter, and produce an edible bread that sustained humanity until we learned how to domesticate it and build the infrastructure to study it until we know how all this works at the molecular level. But they managed to do it without any science or technology.
10k years ago they had actually already domesticated crops and weren't reliant (at least not in many places) on finding wild grain.
Regardless, it was all still done with science: Observation followed by trial and error informed by those observations. Maybe not the scientific method formalized by Francis Bacon, but it's still there in the outlines.
OK, 12K years not ten. I wouldn't call that science- while observation and trial and error necessary, they aren't sufficient. What was done to turn teosinte into maize was more of... a large scale, long-term, unintentional engineering experiment.
I'm not sure you can have engineering without some at least rudimentary approximation of a scientific method. Maybe that's a nitpick though.
Either way, I don't see a fundamental aspect of the scientific method missing from an observation -> trial -> results loop. I also don't see crop cultivation as unintentional, although I'm not clear what you meant by that. What wasn't intentional? Deciding to experiment with planting seeds would have been a deliberate choice. Probably based on some observation that where wild grains were gathered together and and little things fell off of them, sometimes the same type of plant would grow. Followed by the idea that putting those things in different places might produce the same effect. Etc.
I don't think you get from wild gathering in a nomadic lifestyle to settled agriculture without observing, coming up with ideas about what you observed, testing those ideas, and checking the results. That is. A scientific process.
Toesinte turning into maize would may have simply been a blind generations long domestication process, but not that spark of insight and experimentation that led to stationary agricultural societies.
Some considerations on manufacturing — there’s a variety of product quality steps necessary to release batches of medicine. The FDA mandates this as part of GMP regulations. These steps help ensure things like:
* How do I know that every vial has the same concentration of insulin each time? That is to say 1 unit from a vial today and 1 unit from another vial is going to have the same dosing.
* How do I know the insulin is purified? If there’s any host cell protein in the vial, that could be immunogenic and cause bad side effects.
* How do I know that the formulation of insulin in the vial won’t degrade on me at whatever storage condition is stated?
I realize that these tests make up only a small fraction of the price, but there’s a lot of value to purchasing medicine from regulated sources. I’m not against upstart competition against big pharma, but I worry that you might literally kill someone if you don’t include these product quality steps in your process.
> there’s a lot of value to purchasing medicine from regulated sources. I’m not against upstart competition against big pharma, but I worry that you might literally kill someone if you don’t include these product quality steps in your process.
Where are you getting this from? This goal of this isn't to have every diabetic brewing insulin in their garage so they evade the IP police in a distrubuted fasion. The goal is to create open IP needed for creation, purification and quality control that will allow labs around the world to create insulin in keeping with local regulations.
Thank you. This is exactly what we are trying to do. It is difficult for us to get rid of the mad scientist label.
We have a team in fact that evaluate the FDA requirement and looking at what would be the best way to do it.
Also, Open IP means for us that we will share the modified strains which are optimized for the expression of the insulin, and ideally, we will be able to provide scientific knowledge and resources to help the creation of local manufacturing plant.
Off topic question: Is there a database maintained by BioHackers that has reverse engineered some or all of the prescription pharmaceuticals, showing not only the compounds used, but how to make, measure and test them? There are government sites that list all the chemical compounds, but details are scattered all over the place on how to make, measure and test them. Asking as a prepper that wants to stock up on food, water and medications. Doubling or tripling BP prescriptions is insufficient by my standards.
The four thieves vinegar is doing something like that (https://fourthievesvinegar.org/)
They work also on patented molecules and try to reverse engineer proces, and then publish it. (which makes it illegal, so they are anonymous)
I don't know how many molecules they published though.
IANAL, but reverse engineering process is almost certainly not illegal. Don't know where you got that idea.
If they cribbing off a "process patent" then it's not reverse engineering, though, IIRC, for most drugs companies don't bother getting a process patent because they are very difficult to enforce (to enforce such a patent, you need a warrant to go onto a competitor's premises and inspect their process, and judges are very very unlikely to issue such a warrant because if they set a low bar precedent for such actions, then basically everyone is going to start issuing spurious claims), so everyone would rather just build their moat with trade secrets than process patents. Also, I believe if you crib off of a process patent to do a one-off run or research project it is not illegal, only commercializing it is. One (ostensible) point of patents is to encourage sharing and desiloing knowledge and keep things out of the dark so that we can learn from each other.
I will admit, I am no patent expert. To my knowledge, you can patent the process, the molecule, the use of the molecule. I don't know exactly why they are all anonymous on 4 thieves vinegar, I assume it was because of patent stuff. It might be for other reasons. I would believe that showing instruction to produce a patented molecule would be an issue. (maybe not, I don't know)
For insulin, I can assure you that there are patent for processes. Quite annoying.
Ah yes I think I've seen that site posted here before. Last I checked they didn't have a big database, but maybe I didn't dig deep enough into the site. The Download the Apothecary MicroLab Plans go to a status page that says to check back later.
The FDA won't let anything be released to consumers that does not pass their review of the batch record. The whole point of the BR is it's the recipe in totality of how to correctly (which includes quality) make the drug.
The whole point is to open source the batch record.
It makes sense. On the other hand pharmaceutical companies make mistakes also, just on a bigger scale. Also I imagine that when it will be easier to set up insulin small scale production, than more scientists will be able to do innovate and improve the process.
Wal-mart sells insulin for $24.88 a vial without prescription currently.
It's only the newer 'guchi' insulin brands that are crazy expensive. Stuff from 1996 that is compared to in this article is actually cheaper than it was in 1996 (adjusted for inflation).
This is so incredibly wrong - and trying to claim something you know obviously nothing about is hilarious.
The different between NPH (regular insulin) (maybe R too, not sure??) sold by walmart and Fast Acting insulins (Novolog, Humalog, Apidra) is massive.
Fast acting insulins start working at about in about 30 minutes and "peak" at like 2 hours, and may slowly have some effects for another 1-2 hours.
NPH on the other hand, starts working at ~2 hour mark and continues to work slowly until peaking at like 6 hours and slowly degrades away, that means its in your system for something like 9 hours - trying to meal plan around multiple doses of that is unsafe at best.
R is slightly better but still remains and slowly peaks closer to 4 hours.
These are obviously GREAT IF and only IF you dont have access to fast acting. I applaud Walmart for giving access to these, as they are way better than nothing.
Thanks, sithlord. My wife is a type 1 diabetic and it's even worse than your comment suggests, because the different fast acting insulins have a different curve (when do they start working, when is the peak, how long do they have an effect) and our insurance company keeps making her switch to a different "equivalent" formulation because the price to them is lower this month. This means that there's a learning curve, more highs and lows, when she has to switch.
Humalog's patents have expired, as I understand it, but cartel behavior has kept the price high in the US.
The PBMs are mostly owned and operated by the managed care organizations (insurance companies). The insurance companies have profit margins of less than 5%.
My information is from 10-K filings with SEC, and my statement is referring to net profit margins, which are what they are. Unless there is massive fraud going on, managed care organizations are not earning massive profits. If their PBM divisions are, then they are simply subsidizing the insurance division, but it would make no difference to people. The total expense for premium plus out of pocket expenses would not change, it would just shift from one to the other.
One big element is that a lot of large companies and non-profits run their insurance programs as self-insured. They pay the direct costs of the medical care of their insureds, and keep the annual premiums the entire employee-base pays. The "insurance companies" are paid a percentage of the total revenue/claims as an administration fee, so they have incentives to push the overall amounts paid up, not down. Self-insuring eliminates the profit overhead of the insurance companies, but screws the incentives.
There are quite a few big insurers (better known as managed care organizations) competing for business, so the incentives are there to limit expenses so they don’t have the most expensive premiums.
Some insurers (looking at you United Health Care) have wholly owned PBMs. Thus, the PBM is an asset in its insurance trust. Any profit the PBM makes will appear as in increase in asset valuation for their insurance trust, or balance sheet in some cases.
However, insurance margins remain unaffected as the money did, in some sense, go out the door and is no longer in control by the insurer directly. It's not fraud. It's just anti-competivie self-dealing. So, no, it's not profits per se, but rather increased valuation via clever financial engineering.
All the big managed care organizations (better word than insurer) have their own PBM. I would need to read more about how an MCO accounts for assets set aside for insurance, but I would be surprised if insurance regulators are allowing it, considering how strict insurance regulators are.
A quick search shows me that on page 73 of Cigna’s 10-K, it clearly does not have its Express Scripts division accounted for in the “Investment Assets” section, based on how low those numbers are.
It just does not pass the smell test to me. The simpler answer, based on all the numbers, is that managed care organizations are squeezing other entities in the healthcare chain, but due to competitive pressure and upper profit margin limits due to ACA, they are not raking in big bucks.
This is probably true - and I am not here to point fingers - but I will say that the insulin manufacturers are at some fault too, they do just enough to keep renewing their rights to their insulins every time they come around.
You cannot renew a patent in the US. They get a new product patented, but anyone is still free to come along and make the older one. However, I bet there is a ton of expertise and cost required with doing that, and that is what is stopping others.
they "renew" by "improving" their existing product enough to make it obsolete, and to get a new patent. Per the article below this has been happening since 1923
Would it be possible to get a limited amount of the fast acting stuff for unpredictable situations and then normally use the "cheap" stuff? I don't know how this works so I would like some info from someone who seems to know.
Possible, sure, but not ideal. The "fun" thing about T1 diabetes is that every meal becomes an unpredictable situation based on exercise, sleep, stress, etc etc.
Slightly exaggerated, but only slightly: Imagine you could only drink water 6 hours before you got thirsty, but if you drank too much you might pass out (at any point 2-6 hours from now) or if you drank too little you're doing major damage to your body.
Really the only way to manage with that kind of insulin is to live a very, very low carb lifestyle. Its doable, but it limits your variety and leaves you prone to other potential issues.
Not likely, also lets not forget - as a Type 1 diabetic, you also take long acting insuling (unless you are on a pump). So, for example, a pump uses only fast acting insulin - and it gives a small amount (known as "basil") every 5 minutes (+/- depending on pump).
Whereas, if you use pens (or from a vial) with direct injection, you also take a long acting insulin (levemir, Lantus, etc) once or twice a day (they are supposed to last 24ish hours but often people find splitting their total daily dose up into morning and night has better results). And these insulins cost even more than the fast-acting stuff.
It's likely not what your doctor prescribed, it doesn't last as long, it requires you (or your young children) to eat on a very specific schedule, it can't be used with an insulin pen or insulin pump, it's just all around a worse and less effective treatment.
Seems like everything is working as intended? A corporation invests money to develop a better product, and the government gives them a 20 year monopoly on it so they charge a premium and recoup their investment. As a patient if you want to pay the premium for it, you can get the better product, otherwise you can still stick with whatever walmart's selling. It's worse, but it's not any worse than what you'd had if the company didn't come along and invented the better product.
That's not what is happening. It has nothing to do with a patent monopoly or recouping any investment:
FTA:
>In 1996, a vial of Humalog produced by Eli Lilly cost $21. Today, it's priced at $324 despite the cost of production remaining steady.
>Rising costs are nothing new. Insulin prices tripled from 2002 to 2013, and doubled between 2012 and 2016. To put this into perspective, in 1996 a vial of Humalog produced by Eli Lilly cost $21. Today, it's priced at $324 despite the cost of production remaining steady.
If everything is working as intended, it begs the question, what institution intended for patients to die from rationing insulin[0], and why is the USA ok with that institution's intention?
If it was developed in 1996, the patent protection would have expired by now. If the cost of production was "steady", then the question is why is a competitor not jumping in to make and sell something that would earn them a huge profit margin?
Do you doubt it was developed in 1996? Do you have evidence that the cost of production has significantly risen?
Otherwise, you seem to be repeating the old economics joke:
"The young economist looks down and sees a $20 bill on the street and says, “Hey, look a twenty-dollar bill!”
Without even looking, his older and wiser colleague replies, “Nonsense. If there had been a twenty-dollar lying on the street, someone would have already picked it up by now.”"
When there is a claim that there exists an arbitrage opportunity worth billions of dollars, I would consider it common sense to consider why has no one claimed the arbitrage opportunity yet.
The world has many very smart people spending many hours working very hard to find these opportunities, so the likelihood of it just sitting there like a $20 bill on the street, and not being picked up, seems quite small.
I do not know the answer myself, so I am interested in finding out. reddicky posted this:
>Biotech insulin is now the standard in the U.S., the authors say. Patents on the first synthetic insulin expired in 2014, but these newer forms are harder to copy, so the unpatented versions will go through a lengthy Food and Drug Administration approval process and cost more to make. When these insulins come on the market, they may cost just 20 to 40 percent less than the patented versions, Riggs and Greene write.
So it looks like there is some expensive expertise involved and investment into R&D that needs to be done.
Yes there is expertise and capital costs involved, which make it not an arbitrage play. It is more like a cartel, which seems to explain what is going on here, with the 3 insulin producing companies all fixing their prices together (at least in the US)
In theory there is 'nothing' stopping another company from coming along, even a group of Biohackers may try to do something - I wonder if that's been done... :)
The reason no one will pick it up is because there are massive capital investments to get something like that up and running, and the existing manufacturers can just drop their price to compete with you as soon as you get up and running. Now you have to recoup your capital costs in a saturated market, and your competitors can probably make insulin cheaper than you due to pre-existing economies of scale.
I would imagine that even other companies already in the pharma space would be interested. They don't want to play the race to the bottom game with billions of dollars in upfront costs. If anything, it's probably more profitable to make a new form of insulin that you get to patent. Which is how we end up where we are.
Although... I needed to buy a vial of the newest fast insulin in Spain last year without an insurance. One vial was 28 euros, which is much less than people in US have to pay.
The insulin in question is Lyumjev from Eli Lilly.
This is an incredibly stupid comment. Net price in Humalog has decreased since 2014 [0]. The PBMs jack up the list price so they can get their fat rebates.
Eli Lilly's profit margin is double digit, usually around 20%. Managed care organizations (insurance companies), which own the PBMs, have profit margins of ~5% or less.
That is a nonsense talking point from the industry. They use passthrough revenue to distort their profit margin. Express scripts is closer to 15% and CVS is closer to 10%.
If these PBMs are making lots of profits, then they are simply subsidizing losses elsewhere in the MCO. The total costs paid for insurance premium plus out of pocket costs by the end user in the US would not be affected.
You are not addressing my main point which is that these MCO's distort their "net margin" stat using accounting tricks. And yes PBM's are INCREDIBLY profitable. Express scripts made 4.5 billion in net income in 2017. They have never produced a drug that has saved a life.
PBMs are important but they should not be able to put a gun to these pharma companies heads because they control the formulary.
CVS net margin includes their retail business. You can't compare AWS's margin to Walmart's e-commerce margin.
I am not addressing it, because I do not see any further evidence of distortion of an MCO's net profit margin other than what this article claims. Nor would it matter to me unless some MCO executives are smuggling cash out of the country or something.
As a customer, it does not affect me.
In the healthcare business, the flow of money is:
Individual -> MCO (insurance company) -> healthcare providers and drug manufacturers
What does it matter to the individual what portion of an MCO is earning what profit if the net profit margin of the whole MCO is 5% or less? They are obviously not left with a lot of money, their employees are not known to be lavishly compensated.
That doesn't seem too strange when you consider that those two types of companies have different operating models. A drug company is in the business of taking relatively cheap goods and converting them to very expensive goods, in other words adding a lot of value. A insurance company/PBM is mostly in the business of skimming a percentage off transactions.
It is not strange, but it also contradicts claims about managed care organizations earning tons of money. It is not a business you go into to get super rich.
Yes it is working as intended, the argument is that those intentions are inhumane. Can you think of any medical treatments that were developed without the promise of 20 years of limitless profits? I can.
> Can you think of any medical treatments that were developed without the promise of 20 years of limitless profits? I can.
This sounds like it's responding to a strawman. Proponents of the patent system aren't claiming that zero innovation would happen without patents, just that it would be much less. In other words:
No patent system: only inventions from altruistic inventors
Patent system: inventions from altruistic inventors and profit-focused inventors.
Let's say corporations were only promised a 10 year monopoly instead of 20. Do you think their business would collapse, or would they keep trying? If profit-focused inventors could still be motivated by a 10 year horizon, then that extra 10 years only benefits corporate executives and kills patients. So, is the patent system as limited as possible while still encouraging innovation? Obviously not, because pharma companies routinely direct billions of dollars in profit into stock buybacks instead of research or any other actual investment. They can easily afford to make less profit.
It would depend on the project's margins and/or sunk costs. A project that had very little invested in it or is a breakout success might we able to weather a 50% cut in exclusivity period, but a marginal product might not. Most of the already developed drugs are probably going to be fine, assuming that the financing for them was already secured.
>or would they keep trying?
For the projects at the margins? most certainly. That is not to say all private drug development would, stop. If some sort of unpatented-but-super-cheap-to-perfect-but-still-not-patented drug showed up it might still be developed, but in aggregate I'd expect drug development to drop significantly.
I am arguing that there are no marginal projects at current profit levels, and that's why they can spend billions on stock buybacks. There is a point that lessening patent protections would cause companies to cut back, but we are not at that point.
Define fair and unfair. If it was so "unfairly" lucrative, I would have to ask why everyone does not invest in pharma? Why are tech companies where much of the VC funds land?
Perhaps it is because there a huge amount of risk involved?
Type 1 diabetic here. Managing T1D even with the "Gucci" insulins (I use Novolog and have tried Fiasp) is still a huge pain in the butt; you have to give yourself a dose of insulin a fairly precise amount of time before eating, and accurately judge how much you're going to need, which is half science and half wild guesswork. My per-meal dosage requirements vary randomly from month to month -- a dose that would be fine one month is either inadequate or deadly on another month, and the only way to tell if you've got it right is to obsessively monitor your blood sugar.
And that's with the $700/vial insulin... the $25/vial stuff is stone age technology by comparison; you have to take it twice a day, and then eat at two specific times afterwards, or you'll go hypoglycemic (unconscious or maybe dead hypoglycemic, not just the feeling-a-bit-tired kind that people who don't use insulin are familiar with).
The situation right now is that the best and most expensive T1D technology, even the various "artificial pancreas" solutions, still gives you nothing like the experience of a normal pancreas. It would be really nice if the Walmart insulin were a viable long term solution for the cost problem, but unfortunately the negative health effects of older insulin tech are considerable :(
Have you looked into the Warsaw Calculation of calculating insulin? I did it for awhile and pretty interesting. Only real issue is its pretty inconvenient, requires breaking up doses more. But it also takes into account for fats and proteins into the insulin calcuation. I dont remember what, but say your carb ration is 1:10, you would calulate a protein as maybe 1:25 and fat as 1:30 (theres some assigned value is the point iirc - dont use these numbers )
Have you tried low-carb eating? I've been doing it for years and it seems to be an easier method then insulin(type2 borderline when I started, so not exactly the same).
When you eat lots of fat and protein as a T1, you just get a slowly rising glucose that needs insulin and is harder to control compared to carbs with less fat.
T1 is really complex even with a low carb diet, if you don't only eat vegetables, but meatier food.
Yeah, T1 is pretty much just a pain whatever you do. Low carb does make it quite a bit easier, and I imagine would pretty much be the only safe way to eat if you were using a non-rapid insulin.
Unfortunately (doctor's orders) I also have to cut back on the cholesterol, which seems to be very high in all my favorite low-carb foods :( It's a constant experiment; it may turn out to make more sense to eat more fat but take statins, but I need to wait a bit longer and see how my lipids look with the current diet.
(BTW I'm actually doing fine -- pretty decent control/A1C -- but I had to rant in response to the Walmart insulin suggestion above!)
Some other things that raise your glucose and you need insulin:
- waking up, liver produces glucagon
- stress at work, hormones going wild… including glucagon
- weather changes, when it is cooler you need more insulin
- you get sick. 2-3x insulin for me
- liver just having a normal glucagon production, that needs insulin without you ever eating anything
Nice that you have your A1c in control. Mine is 5.8% without too many hypos after 26 years of having T1. The tech I need for this costs a fortune without insurance, but at least I can finally live a normal life without nasty surprises every day.
A friend had insurance problems for years and often had to use Walmart insulin instead. He's now going blind, and his doctors suspect that's why. </anecdote>
The hard part is getting doctors to offer prescriptions for the cheaper brands as an alternative. A lot of doctors will prescribe the most expensive drug simply because they believe or know that it is better in some way without regard to it's cost.
It's changed a lot recently as doctors have become more aware of the cost of these drugs. But you still have to self advocate for less expensive drugs. Less savvy people often have trouble getting transparency into drug costs. Often even the doctors can't get a straight answer on pricing and insurance coverage.
It has been many years since pharmacies have been allowed to substitute brand name medications with generic medications. In fact, doctors have to write "dispense as written" if they want the patient to only get the brand name medication they prescribe.
Additionally, managed care organizations (MCOs, commonly known as insurance companies) do not pay for brand name medications just because a doctor prescribes them. If the MCO is aware of a generic option, then they will only pay for the generic or they will ask the doctor for a "prior authorization" to justify the use of a brand name medicine (such as the generic version not working).
The pediatricians I have visited in recent years even have the MCOs' formulary available for the patient in their systems, so they can see which medicines need a prior authorization and which do not so there is no time wasted on figuring out what the MCO will pay for without prior authorizations.
> A lot of doctors will prescribe the most expensive drug simply because they believe or know that it is better in some way without regard to it's cost.
This is so obnoxiously common across every profession.
People are willing to piss away other people's money on "the best" without even telling them what the options are.
True! However doctors often don't know this or simply don't think to mention it. In addition, self medicating with OTC insulin can lead to poor outcomes. With proper training and care it can be a powerful tool for uninsured patients. However, insulin can be extremely dangerous leading to ER visits and insane hospital bills.
Every time I try to wrap my head around this stuff. How to fix the problems with our current system. I keep coming back to socialized or single payer health care.
Sure the current system works okayish for people like me. Insured and employed. But for my friends and the people I meet on the streets or the grocery store it's a nightmare. There is real suffering and death caused by no access to adequate health care. Even basic preventative stuff like diabetes care and checkups is missing.
Walmart insulin is not lispro/glargine, it is R/N, which is a different formulation. Treatment of type 1 with R/N is associated with significantly higher mortality, A1C, and complication risk, and, of course, much lower quality of life.
Bear in mind: when you mis-dose insulin, your blood turns into acid.
No endocrinologist would ever recommend treatment with older insulins over the new stuff. The only way it happens is because of cost.
This is like saying a car and a bicycle are equivalent means of transportation. Sometimes a bike is the right solution for some people and a bike is usually better than nothing but it’s really not fast enough to be a practical solution for most people’s daily needs.
Edit: Perhaps high speed internet vs dial-up would be a better analogy to spare us the comments about how bikes are actually better than cars...
Goodrx shows lispro generic $48.85 per vial. Humalog 'guchi' is $142.55. If you're fortunate enough to have diabetic retinopathy and can't read the tiny print, the larger kwikpens are only $270.28. Lets not even get into the real guchi brands.
Patient outcomes for the insulin aspart pens and the vials of generic insulin at Walmart are so different that many doctors refuse to prescribe the cheap stuff except as a very last resort.
There's no simply substituting. These are two different brands of a generic statin pill or something. Although it's all insulin, these are very different drugs. The dosages for the same insulin in the same patient can vary, and the calculations or charts for what to take when vary across types of insulins. The handling instructions vary. There's different patient training for a pen vs. a vial and syringe.
There is no substituting but also no easy comparison of how much worse the regular stuff is, since the population using R is often underinsured and unable to afford other elements of prevention and care.
That fixes the pen issue, but it's still not the same insulin most doctors prescribe and can't be easily substituted without medical consultation. Having it available inexpensively and without a prescription is a compromise, per Novo Nordisk themselves.
I really wish this would be a higher priority for the current class of billionaire philanthropists: open source science.
Medical research guided by the idea of preventing disease rather than creating expensive life-long treatments, and prioritizing the diseases that cause the most amount of suffering rather than present the best opportunity for profit. And not just medicine, but just about any industry could benefit.
Wall Street Smart Genius types have long held that curing disease is bad business, managing symptoms over the entire lifetime allows them to extract more capital out of the cattle.
So, if you're looking to cure something you're going to struggle to find funding.
> Wall Street Smart Genius types have long held that curing disease is bad business, managing symptoms over the entire lifetime allows them to extract more capital out of the cattle
Nobody tell the multibillion dollar biotech industry…
And in case it needs to be pointed out, no, cures are massively profitable. If someone has a cure for a presently untreatable disease you will get money, you will make money, everyone will make more money and everyone will be better off.
> everyone will make more money and everyone will be better off.
Not the people who are currently making bank off of palliative care for that ailment. This absolutely creates perverse incentives that, while not ubiquitous, are hardly uncommon.
I would argue the vaccine for Covid is essentially a cure. And the economics aren't that good. People got it once. They may or may not take a booster every couple years. And that is for a disease that everyone was impacted from.
Meanwhile, a drug like viagra can be consumed several times a week for decades.
I don't think its pharma execs are sitting their blocking cures, but it is true that they will looks at risk/reward when deciding. If most drugs only have a very small chance of being approved (lets say 2%) and costs billions of dollars to move through the process - of course those that are needed over and over are going to be funded through research more.
I'm going to need see some numbers on this statement. Because from where I'm sitting, the potential market is every human on planet earth, which is a pretty large amount of sales.
Production costs of mRNA vaccines, as well, is quite low, with much of the cost spent so far spent on scaling.
Yes, I do take issue with the government granting monopolies to private entities with taxpayer funded research. But not all of the funding for all the treatments I mentioned, which are clearly cures and not meant to bleed people until they die, came from government.
Sometimes the pendulum swings too far towards cynicism.
Then they get a cancer treatment, that was likely partially funded by the government via grant or tax benefit or medicare graft but fully owned by the private company, they are charged tens of thousands if not hundreds of thousands of dollars even though they have insurance, then mostly die anyways, because although cancer treatments are much better, they are still in the stone age.
And their family than learns who actually funds cancer research: they do.
It's funny because your statement was supposed to support the idea pharma only do good things but instead it exactly shows the failure mode of capitalism in medicine: when you get sick, its very often that you do not have the time or capacity to be a informed consumer and the entire premise of capitalism breaks down.
Can someone explain in layman's terms why there is no competition on this market? As insulin is so cheap to produce, why can't I just get my own product approved and sell it?
There are crazy patents throughout the entirety of the insulin production pipeline. Some of these being extremely absurd such as patenting the pH of a buffer for specific protocols! I volunteer for the Open Insulin Foundation on/off when not too focused on my research project and it's basically how can we come up with a roadmap to making this decentralized insulin without violating any existing patents. An added layer of difficulty is like other have mentioned, engineering Ecoli to produce the homolog as well as developing from scratch the devices for extraction and purification (think hplc). Again, these need to be made from scratch as to not violate any patents. At least in the U.S., this is why there is no competition in the market. There is also a significant price barrier as you need to bring up your production to GMP standards which means you need a state of the art clean room and multiple roles to supervise the production of the product every step of the way.
Both too long time of life, and too easy and cheap to extend.
Most importantly, it's a while set of single thing patents which means you need a thick, expensive cross licensing agreement most of the time. Even finding out which patents you need is hard, and then the patents are written in a way that nakes them hard to use too, including incomplete in crucial details.
It's a mockery of the original intent of the patent system.
We figured out how to patent everything in software by just adding "with a computer system" to it, so I'm sure we could figure out how to patent novel combinations of these procedures by mixing in "in microgravity".
That does not work, because for most of the biochemical postprocesses (which are critical) microgravity would have completely no effect and as such patent office would be liable to reject the patent as redundant.
Yes! The Open Insulin foundation not only has volunteers with a biomedical background, we have volunteers from many other backgrounds including lawyers that help us try and challenge existing patents. Again, others have said that manpower might be better invested in openly challenging the monopoly that U.S. companies have on some of these patents in court or by appealing to our congressmen. However, I believe that there’s no reason not to do both in parallel. My scientific training can only take me so far and i’ll happily help a project like this if it can open up a new source of affordable insulin in this country, but believe me, I know that at the root this is a legislative issue.
They're specifically targeting small molecules, the infrastructure for proteins is different, and probably won't work with their model (subcontracting small compounding pharmacies to make the drugs)
Similar to a pulse oximeter that measures oxygen saturation non-invasively, is there some research on finding similarly the level of glucose in the blood, etc?
You don't need new laws to deal with corrupt business practices. The fact that cheap off-patent insulin isn't available in the US is clear proof that the pharmaceuticals are all colluding together to maintain high pricing. Otherwise free market forces would take over and someone would sell what the rest of the world gets, siphoning off sales from medical tourists going to Mexico and those who want off of expensive alternatives. Conveniently the FTC looks the other way. The American government in inaction.
I was not suggesting that we need more regulation necessarily. It's a problem of law in that it's entirely made possible (and incentivised) by laws. Patent law and laws governing the development, marketing, distribution, and crucially import of medicines.
Yes, if you make a mistake, you could easily overdose, hypoglycemia and die. Or underdose, and become hyperglycemic and enter an altered mental state where you'd be unable to function normally, or lose connection with reality.
I don't think it's reasonable to expect everyone who takes or buys it, to be able to determine if what they need to inject into their body to survive is safe and functional. So yeah, I do think there should be laws and limits on what qualifies, and who's allowed to make it.
Do I think a large corporation is the only thing able to do that? No, but I suspect that it'd be hard to prove you can make the minimum guarantees that it's safe from the first dose to the last. And that you have resources to attempt to compensate anyone you hurt if you do break those guarantees.
Why not allow patients to buy generic insulin from overseas (from India for example) ?
If I could just you know, ask a friend of mine to fly to India and bring a monthly supply of cheap India made generic of Humalog, that would be great, right?
and if insurance company kicks in a few bucks for me, that would drive down the cost of care for insurance company as well
The FDA heavily restricts import of foreign drugs. That's been the case since the Thalidomide incident in the 60s. Essentially drug manufacturing is a closed market, not a free one. Even if one gets rid of the incumbents like Pfeizer or AstroZenica, the same system just breeds the same perverse incentives.
This is sort of meta, but it's cool to see Free Think popping up here. It's a great publication that I think would really be of interest to this community.
More germane to the article, it will be interesting to see what happens over the next 10 years as bio-tech becomes more accessible to hacker types and hobbyists.
in 1996 a vial of Humalog produced by Eli Lilly cost $21. Today, it's priced at $324 despite the cost of production remaining steady
Honest question, how do pharma executives walk the streets? If I was engaged in activities that vile I'd be terrified of being murdered by a vigilante.
There is no stranglehold. It's being manufactured for peanuts everywhere that is not USA.
That country suffers from no central negotiating body to drive down the price, and a manufacturer/insurer virtual cartel. In other countries, government either negotiated a good price, built or subsidized a quality factory.
The remaining people who have problems are in parts of global south for various reasons, some of which involve exploitation and others bad government or warfare, leading to lack of resources and experts.
Why take the risk in selling something like that? You're never going to be able to make money on it. Or did you mean people should just make their own?
I simply don't understand the healthcare system in the US. Its meant to be a free market, yet insulin costs a ridiculous amount. However Opioids and synthetic opioids are cheap as chips.
To put it into context, In the UK the NHS buy Insulin at <$35
you can see the prices here: https://bnf.nice.org.uk/medicinal-forms/insulin.html They come from the same companies and are produced to the same standard. How can a bureaucratic "socialist" care system get better price, and a much better availability than a "free market" system. (thats rhetorical, I know why)
Given the number of non and under insured, I just don't understand why its not swinging elections.
Generic Insulin Lispro is currently ~$50-60 per vial in the US, without any insurance or assistance from the manufacturer (though you do have to understand the system and go to specific pharmacies to get that price).
The reason it's not a big issue in elections is because lots of people don't vote.
And every state administers its own Medicaid system under a different name. Lots of folks don’t even realize that their free healthcare is mostly coming from the feds. In AZ, I had to explain this to several friends that depend on AHCCS.
Read 'The price we pay' if you want to understand the US healthcare system.
Most of the 'socialist' countries don't pay for R&D on drugs; US consumers do. They pay a marginal price based on production cost, but almost none of the fixed price investments in efficacy, safety studies etc.
The US system in no way resembles a functioning market. It's a byzantine spider web of regulatory capture, patent abuse, bad incentives and inertia.
The real fundamental problem here is very easy to fix. We need to completely eliminate patents from our legal system. Doing so would fix the problem with insulin, as well as the problems with every other drug and with software and with tractors not being repairable and many other areas.
As an observation, The UK, USA, Canada and Australia are all in the top 10 for type-1 diabetes incidence in the <14yo population, along with Finland, Sweden, Saudi Arabia, Kuwait, Norway and Denmark.
Only the USA imposes private health cost burdens on the diabetics (from my quick scan of national health info on the web)
Math is pretty simple if you have 3-4 producers off essential product protected from external competition by patents.
In this case better to avoid competition and increase price 10x than compete in hope to increase market share maybe 2x-3x.
What's the actual situation there? I have read that cheap insulin for example is available at WallMart, but for some reason the price of insulin seems to be a huge issue.
There’s different kinds. IIRC the cheap stuff and Walmart is just that, cheap. It’s fast acting, and varies in how it reacts in the body.
Our real issue here is that there is absolutely no incentives to control costs.
You’d think our ins companies would do it, but I’m practice, they end up negotiating sweet deals with the drug manufacturers. say med X @ $1000/mo msrp, but the ins companies negotiate it down to $400/mo. The drug company makes out like a bandit, and the ins people get kick backs for buying from the drug co, and passes on the costs to the insurance buyers.
> It’s fast acting, and varies in how it reacts in the body.
I believe they offer R (short acting / 2-5h), N (medium), and L (long acting / 24h). The problem with the older insulins isn't so much that they're faster, it's that they're less "specific" (from my experience). A newer short acting insulin (Apidpra, etc) has a spike in the 15-30 minute range and the spike is steep and the tail (while up to 5 hours) is low. Whereas R peaks in the 30m-1h range and the peak is low and the tail is much higher. As such, you need to plan ahead much better for your eating. It's frustrating, but not horrible. The N and L have similar problems (L is the reverse, where you want a tail equal to the spike, but it isn't).
The newer insulins a just much more convenient and require a lot less planning of what you eat and when... and not as close an eye on your blood.
If that's actually the case that puts all the "You're literally killing us with expensive insulin prices" people in a very negative light. At best they're ill-informed, at worst they're being intentionally deceptive to achieve political aims.
I have to ask, are you suffering from a Type 1 diabetes? If not, at least for me, this answer kind of misses the point completely. Type 1 is a hell to manage. It is REALLY hard.
Like I actually use an open source pancreas to control my glucose levels so now I can sleep every night without having to worry about dying. This is in Europe where the insurance covers everything and prices are cheaper than in US.
Using the Walmart insulin makes everything much much more complex, and even for the smartest of us, even with the best possible insulins, managing T1 is a HUGE pain and can kill you quite fast.
I do have type 1 diabetes, and I lived on R/L for over a decade. The point being made here is
> The high price of tier 1 insulins is killing people
Is (more or less) a lie. While
> The high price of tier 1 insulins is making people's lives considerably worse and their diabetes harder to manage.
Is (more or less) true.
When you try to push for change and use, as part of your argument, a lie, you sabotage yourself. People can point at what you're saying and, ignoring the validity of what you're trying to achieve, say "you're lying". That's bad.
The truth is that there are good reasons why tier 1 insulins should not cost as much as they do, not by a long shot. And destroying your own progress towards changing things is counter productive. Just don't do it.
It is not a lie if you think about real human behavior, rather than a theoretical rational automaton. There are real, documented cases of people who were prescribed insulin they could not afford, tried to ration it, and died as a direct result. Maybe their doctor told them not to use it, or they didn't live near a Walmart, or they didn't know it existed. Maybe they tried the Walmart stuff and almost died because it's so difficult to manage, so their doctor told them to switch back to the best treatment available. I promise they did not die to make a political point.
It is simply untrue to say the high cost only forces people to use the cheaper Walmart generic. That isn't what happens. They ration it, and sometimes they die.
Finally, it doesn't make sense to say that the high price is making diabetes harder to manage, but isn't killing people. That's like saying speeding doesn't kill, it just makes the car harder to manage.
> One in four patients say they’ve skimped on insulin because of high cost
> say they've
^ is the key component. I expect the vast majority of those people had a choice, and they chose not to take it. A poor choice, and a choice they shouldn't have to make, but a choice nonetheless.
The point is, if you're going to fight for positive change, use an argument that can't be trivially dismissed because it isn't true. Fight effectively.
Yes, why did they choose not to take it? Try to empathize with these people. Why did they do something so dangerous? Then follow it one step further. In the case of those that died, why did they die? What factors contributed to their death? If the price of insulin had been lower, and everything else was the same, would they have died?
I would argue these two statements are equivalent:
- My patient was killed by the high price of insulin.
- If the price of insulin had been lower, my patient would still be alive.
I suspect that you accept the second statement, but not the first. What's the difference?
To me, it's the difference between "is a requirement for" and "is the cause of".
- People drive cars.
- Cars are car jacked.
- If people did not drive cars, carjackings could not happen.
- People driving cars is a requirement for carjackings.
- People driving cars is not a cause of carjackings.
I understand that it is possible and truthful to argue that people driving cars is a cause of carjackings; it's just not my view of the meaning of those words.
By claiming that the companies are colluding and have raised the price, the charge is leveled that the companies are behaving immorally.
When people learn that the "old insulin" and "new insulin" are completely different products and that "old insulin" is still available at a low cost, the narrative and goodwill is shattered.
People hate being lied to and they hate being manipulated.
If you want to have a discussion that we should make the "new insulin" available for at low cost of for free, that is great! We can talk about the cost to manufacture and to develop drugs.
There are many smart people here and around the world, when we put our minds to a problem, we can find a solutions.
But by not acknowledging and downplaying the time and effort that companies and people have put into the "new insulin", then you are cheapening the work they have done and are signaling to everyone that you would do the same to their time and effort as well.
Saying that cheap insulin kills people seems like a hyperbolic, but essentially true statement.
It's well known that you need to keep all sorts of things under control with type 1 to avoid long-term health complications. Blood sugar is the most obvious.
I watched my father manage his for decades, starting in the 1980s. The technology improvements were interesting - his first insulin pump (about the size of a VHS tape), the custom software to data-dump his glucose meter, "supply-hacking" to keep the infusion sets affordable...
He still had management challenges despite being a dedicated, disciplined, marathon-running Mormon on the leading-edge of treatment. He was fortunate enough to be involved in the DCCT/EDIC trials at the University of Washington, and took the early lessons about future complications very seriously.
You make Diabetes harder to manage by removing modern improvements to the standard of care, and you are certainly going to see increases in deaths and severe negative outcomes.
What you've said is true. Refusing to use the older insulins is what is killing people. Having to use the older insulins is shitty, and it shouldn't be happening, but it's not the thing that's killing people.
However, actually _saying_ that tends to get people up in arms, harassing you about how it how it shouldn't be necessary for people to use the older insulins, and how the newer insulins shouldn't cost what they do. Even though everyone actually agrees with them and they're arguing against a point that nobody it actually trying to make. It is... frustrating trying to get people to understand that you agree with them, but you're talking about something different.
I had this exact discussion with one such person yesterday, and I was trying to explain that they are sabotaging their own goals by misrepresenting the issues. And that I WANT them to succeed in changing things, but they're making it harder to do so.
Edit: You're already being downvoted for stating something that is obviously and undeniably true, because people are not bothering to understand what you're saying. I'm sorry for that.
Having to use the older insulins is shitty, and it shouldn't be happening, but it's not the thing that's killing people.
In a way it is killing people, blood sugar control is much easier with a mix of the newer insulins, and patience compliance is much higher. This directly translates into better quality of life and lower disease burden from diabetes complications.
No one can argue that pharmcos shouldn't be paid for R & D that increases quality of life, in civilized countries the taxpayer should and will pay for your medication if it's an improvement over what's already at market.
But here people seem to be arguing that if you can't afford anything else there's still Walmart short-acting Humalog, and you get to bear all the risk, and that's just fine.
I found some references for "old" versions that claim price increase from $17 in 1997 to $138 today, another from $21 to $255.
Going by inflation only those would be around $30-40.
I don't know how much a typical diabetic needs per month (I imagine it varies) but I could see that being a problem for a lot of people if that is, say a monthly supply.
About $25, that last I checked. The ones you're talking about, I believe, are the "newer" ones (which are not very new). The prices of those have shot up over the years (in the US) for no good reason. It's shameful.
My understanding it that they are out of patent, but regulations make it hard for new players to enter the market. Since the number of companies making them are so limited, even the generics cost a lot.
For example, Basaglar is a "generic" of Lantus, but it's still expensive.
> Basaglar contains the same kind of insulin as Lantus (insulin glargine), and while it is cheaper—Basaglar costs about 15% less than Lantus—it is still expensive, with a cash price of around $450 for a 30-day supply.
Unlike normal generics, the bio-similars need to go through their own clinical trials and prove they work the same as the original. They can't just "use the same ingredients" and release it. Mind you, that doesn't explain the extreme price markup, but it does explain why these "generics" don't follow the same "85% cost reduction" of normal generics. They still have, effectively, a costly R&D phase.
I understand that argument.I hadn't thought of the issue of insulin being a biologic, so true generics aren't likely, hence biosimilars. None of this justifies a 10x+ price increase on the same product over 20 years of course.
By the way that same site had an interesting article breaking down costs normalized by insulin unit
By that table and some assumptions about approx 40 IU/day it looks like the cheapest you could get away with at full retail would be about $120/mo, assuming optimal usage etc. The most expensive version would be at least 5x that.
It's extremely hard to manage your health with old insulins because they're so much less precise. Imagine if you were programming but your keyboard works such that any key you type might be +3/-3 key presses actually. Except in the case of diabetes, this results in the loss of body parts and blindness.
The people who can least afford healthcare also have the most external constraints on their work and life, making it the most difficult to make good, non-harmful use of older insulin in the long term.
There are plenty of cases of people literally dying because of difficulty managing insulin due to cost. It’s nice to say other low cost forms are available while handwaving away actual deaths as well as accumulative long term damage from difficult insulin management.
It's the same with basically every other campaign that wants to grab headlines. It literally makes no sense that insulin prices are killing people and it's unavailable, and a basic amount of research shows that yeah indeed, it's clickbait intended to hook you into a more complex discussion.
I pay zero attention to people and news sources that repeat that behavior more than once. Lead with the truth.
You are a prime example of WHY that lie is bad. The discussion they are trying to drag you into is an important one, and well worth having. However, by starting out with a lie, they are driving you away before they can even start the conversation with you about it. A conversation where you might agree with them.
That's context I've never gotten before. Obviously there's a nice convenience benefit built into this product that a company has created, they should get to charge some markup for that.
I wonder how different the production costs are though, my understanding is the costs to consumer are greater than 10x
The difference with the old insulin vs. the analogs is that with the old ones it's really easy to lose a toe, leg, kidney or get blind. With the new analogs it's possible to control your glucose levels so that you can stay healthy and get old.
Source: a T1 diabetic, used all possible insulins in my life. Very happy in Europe.
They also tend to have a more reliable absorption curve. I take both Novolog (short acting) and Lantus (long acting), which are the newer insulins. Lantus has a more predictable long acting curve than the older L did, even though I take it in a 12 hour cycle. It rises not so much like a bell, but more like a plateau, I guess it a better analogy. At least for me. The L really was a pain for planning, especially when physical activity was involved, as it would shorten the bell curve.
On a related note... if you can afford a CGM (continuous glucode monitor), especially one with alerts (like the Dexcom G6), I wholeheartedly recommend one. They are life altering for a type 1 diabetic. Being able to check your blood sugar by just looking at your phone (or separate receiver) is very convenient. I check my blood sugar 100 times a day, instead of poking a hole in myself 10 times a day. And I can (mostly) rely on it alerting me if my blood sugar gets low (or is going to get low soon). I cannot stress enough how much it changed my control of my diabetes.
Admittedly, they're not cheap w/o insurance, which sucks. But if you can get one, so do. You won't be disappointed.
I keep on trying to get one, but being well controlled, the ins cos won't approve it. And its pretty spendy out of pocket. My biggest use case would be an alert that my glucose levels are tanking while exercising so I can do something about it before I drop out. I find myself not doing things like long bike rides that I'd really like to do because of it.
You should be able to get the Libre 14 day sensors for about $120/per month (2 sensors) without insurance. I've been using it for about a year and it has been a huge game changer for me. I've been on insulin for about 23 years. The Libre doesn't have alerts but being able to tap your phone to your arm to test your glucose makes a big difference in how you test/monitor even without alerts.
The alerts (of the G6) are certainly desirable (amazing). But, as mike notes, even just being able to check your glucose with 0 effort... just changes everything. You wind up checking it so often that it's more than just checking it, you get more of a feel for how your body is reacting to your food/activity/etc. I can't say enough positive things about it.
Not actually the question since countries with modern healthcare systems provide all types of insulin at an average cost per unit that is roughly 1/10th to 1/20th the cost in the United States (cheap vs. expensive is an over simplification).
No, it is the question because countries with public health systems often don’t pay for the latest generation of drugs, since they don’t feel the extra cost is worth the benefit.
My comment answered that "countries with public health systems" actually do "pay" for the "latest generation insulin" (i.e. the price for the "latest generation insulin" is still a tiny fraction the cost in the United States).
Just repeating the question, when I gave you the answer, isn't very productive.
We should ask what are the outcomes that these systems produce, not how new the drugs are.
A cutting-edge healthcare system plagued by inequality and extreme costs can produce worse results than a more efficient healthcare system which is not as high-tech.
The entire hamburger market is for profit, but that isn’t a problem as I can buy good hamburgers at many different price points. The issue is that the industry is controlled by 1% of the population who have exclusive rights to decide what you buy, and a government agency that limits the hell out of who can sell anything in the name of safety.
When Europeans can pick from 5 different spring loaded epinephrine injectors and Americans can only legally buy one from a specific manufacturer, of course Americans pay 5x as much.
In plenty of places around the world you can buy all humulin you want without a doctor or the FDA for $30 vial.
If Hamburgers were required to survive I’m sure you would see the same problems.
If the state was the single largest negotiator for purchasing hamburgers and representing tens of millions of people odds are you would have more competitive hamburger supply bids.
The situation is that Type 2 Diabetes has raised the demand for insulin. More demand raises prices.
The thing we can't talk about without risking cancellation is that nearly all Type 2 Diabetes is preventable. In other words, the choices of the many have a significant negative impact on those (i.e., Type 1'ers) who don't really have a choice.
the EU has twice as many diabetics as the United States yet they have no "shortage" or "demand" related problems.
Our situation has nothing to do with demand and everything to do with corporate greed. Many western European countries empower their governments to set upper bounds on the costs of medication to reduce the ability of pharma-bros to make disgusting amounts of personal wealth off the suffering of others.
the increased demand for insulin is not why the price is higher.
Insulin is made in massive facilities in large batch runs. Making 5X to 10X is basically cost of materials, which haven't really increased enough to justify the price increase.
This is (mostly likely) a rent-seeking situation where a few providers who are allowed in the market are milking it for all the profit they can.
I'm the downvotee. I think they understand economics. Who doesn't? What they refuse to admit is:
1) Healthcare is a limited resource, like anything else.
2) Prevention, which few if any "leaders" highlight, is a viable alternative to healthcare price increases.
Are there there some nefarious undercurrents? Yes, of course. But to blame all our ills - and remove diet, lifestyle, etc. - on ever increasing demand only makes the current system stronger. People who believe they have no control aren't part of the solution.
I think we all understand that Type II is preventable but I don't think that's the main focus here. There are plenty of folks who have Type I that can't afford Insulin and have to ration it causing harm and additional costs in healthcare. It's slow mass murder for Type I diabetics who can't afford their medicine. If you believe that it is a supply and demand issue why does the same Insulin cost 80% less in a country like Canada and before you say it's subsidized, it isn't. An American can buy it for substantially less if they can get a prescription from a Canadian doctor.
> There are plenty of folks who have Type I that can't afford Insulin and have to ration it causing harm and additional costs in healthcare
Exactly. The preventable T2D is driving up demand (read: prices) for both T1D and T2D.
I don't know about Canada. I do know about supply and demand. We all do. In the context of healthcare it makes no sense that ppl abuse their health and then expect prices to fall.
What if I were to tell you the the Insulin for Type II diabetes is $35 at Walmart and the Insulin for Type I is $380-$500. By your reasoning shouldn't it all be expensive?
What you fail to consider it that the company that controls the particular type of Insulin that Type I diabetics require is charging 80% less in Canada than in the USA with everything else equal.
Manufacturing - not just the product - is a resourse as well. Going to the doctor is a resource. Health insurance employees a resource. Etc. We keep puttingg more and more demands on the resources and...want prices to fall?
Our food system is sure rigged to make us fat. But then, in my case, what was it that triggered the t2d? Was it the family genetics (both parents are t2d in their old age), the over abundance of sugar in the std American diet, the stress caused by abusive relationships (parents suck, plus ex wife made my life a living hell), or the adrenal tumor?
Never claimed scarcity. Only that as demand has increased - and it has significantly - so has price. It's basic economics. Unless there are additional economies of scale from that multiple then prices are going to increase. This isn't about insulin. It's simple economics.
Sorry, but regular people don't make "campaign contributions" of any noticable size, so all we get back is a form letter acknowledgement based on whatever box you checked for subject.
Big Pharma, Big X and Big Y, on the other hand, "donate" enough "campaign contributions" that the campaigner can all but ensure (re) election based on recent name recognition to get the nomination, then counting on "their" voters being unable to vote for the opposite party even with the discovery of a live boy or a dead girl.
Respectfully disagree. I live in a smaller US state and I’ve emailed my representatives and received a personal reply from both of them. One actually engaged and we politely discussed a public policy issue back and forth in an email thread. More often than not you can walk right into their office and meet them if you’d like.
And did meeting them shift their position on an issue where the opposition is a massively powerful and wealthy industry that spends millions on lobbying efforts?
I hazarded a guess that a bit more than 500 people suffer from diabetes in the US -- more like 34 million. If you could get one in a thousand to agree to take political action, that's 34,000 people.
What always amazes me is how much this is tolerated in the “Land of the free”. At what point do Americans stand up for democratic principles?
This pathetic “we can’t do anything” attitude will be how democracy dies.
If my electoral district was gerrymandered or corporate donations through PACs we’re allowed in Canada I would be planning protests instead of typing this. Our system is far from perfect, but I have a hard time imagining a scenario in which the public here would passively accept many of the things we can see to the South.
Why is there so much apathy towards these issues?
Shouldn’t the fairness of the democratic system in the US be the #1 issue for both Democrats and Republicans?
When you're told you're number one your whole life, you don't go anywhere else, and your religion and patriotism are joined at the hip, why, there's no reason to change anything.
I can't find the link now, but something that really opened my eyes on terrifying PACs are was someone pointing out how they manipulate the political discourse without even spending a dime. They just sit there on a gigantic warchest and send out gangster-style missives like "hey it sure would be a shame if you supported X or Y and we had to drop $10M on pummeling you with primetime TV ads in the week before your reelection."
This kind of influence is completely untraceable through all the normal disclosure mechanisms since no money actually gets spent. And worse still, it offers enormous leverage— once you have that war chest, you can use it to issue hundreds of threats and only occasionally have to actually follow through.
It's just a completely different ballgame compared to a "normal" campaign finance option that directly spends donations.
Are you sure? Pretty sure they can. Either way they can donate huge amounts to PACs, create their own PACs, run ads, etc. Bribery is pretty much legalised, it's ridiculous. See Citizens United v. FEC for example.
The whole point of a PAC is that they don't donate to the campaigns directly, but rather exercise their free speech to supply the public with "information" about the candidates.
The US health care system combines everything bad about government-run health care (slow progress due to heavy regulation, layers of bureaucracy, government-enforced drug monopolies) with everything bad about free-enterprise health care (inequality, market price fixing, uneven quality, lots of quackery at the edges of regulation).
We need to pick something. If we're going the free enterprise way we need competition, price transparency, quality and outcome transparency, more open markets, and much lower taxes. If we're going the state-run or state-insured way then we need to whole-ass it and vertically integrate and drop the state-backed private insurance hybrid nightmare.
The US does this pessimum thing all over the place. We are taxed almost like a more "socialist" country (unless you are rich enough to offshore and play tax loophole games) but do not get the benefits of one. Either cut my taxes down to Costa Rica levels or give me benefits at least as good as Canada please.
Every time I’ve dug into it, modern nations which enjoy a much lower cost per capita coverage (which the US is a major outlier) basically have a government mechanism to set prices for drugs and health services.
There are no free market health systems in leading economic nations (unless maybe you take a very small niche corner of the systems)
> There are no free market health systems in leading economic nations
That also does not exist in the US and hasn't in more than half a century. The US could hardly be any further away from a free market in healthcare. It's hyper regulated, and hyper dominated by government programs (Medicare, Medicaid, and dozens of other programs and agencies).
The US healthcare system is controlled top to bottom by rigid, strict government regulations and oversight. It's the way it is precisely because there is no free market at all. The corporatist interests like it just the way it is, and work with the politicians to constantly maintain that highly regulated environment: it's regulated in their favor, exclusionary of nearly all potential competition. And it's insanely expensive to try to start anything in healthcare, which favors the incumbent further.
Try starting a hospital or opening a clinic. Try becoming a doctor. Try getting a drug to market. Try getting a medtech device to market. Hyper regulation every direction you look.
My point is that it's seems a little optimistic to think that a free market for healthcare is an adequate solution, given that no free market healthcare system exists anywhere at scale. I think some markets are simply inappropriate for free markets - particularly one where services are by definition specialized and market feedback involves failures in critical life risking situations.
The parent was fairly pointing out that healthcare in the US is not a free market. For one there is zero price transparency let alone competition. For another there is the insurance industry which is both heavily regulated and state backed. Health insurer market is similar to the wired ISP market.
We don’t really know what a true free market would do with modern healthcare because as you say there is no such thing. Personally I think it could work for middle class and above but would leave a big coverage cliff down below because it’s not profitable to insure or treat the really poor.
The question is whether real transparency with price competition and efficiency gains would make it cheaper to then add a safely net for the poor.
I've heard that Obama was reluctant to push harder for a public option because the health bureaucracy is such a massive employer. If true then we're basically dragging along a counter-productive boat anchor that eats a ton of our health care spending as a back-door jobs program.
They dropped it to woo one moderate Democratic senator (Lieberman), who was basically the Manchin of his day. Without his vote, it would've gotten filibustered to death.
You're absolutely right that either would be better than the current situation.
The issue, though, is not that it's half-assed and fucked up. It's working by design, to use legislative schemes to funnel money to incumbents and friends/donors, while still supporting the "free market" ideology, when really it's just regulatory capture.
The system is designed for graft, and it's working as intended. Those with the power to "fix" it won't, because to them it's not broken at all.
The US has the same problem in telecommunications, war/defense, and medicine. The largest vendors become integrated with the budget- and policy-makers, and the whole system exists to extract maximum value from the consumer class.
What we need is a focus on prevention. A significant amount of the system is devoted to preventable conditions. Lower the demand and prices will naturally come down across the board as resouces get redistributed, etc.
But as it is, insulin is high demand and increasing. Prices simply don't fall when demand increases.
If your question is truly serious, the answer is: nothing. It's almost certainly impossible to fix the US healthcare system given the enormous number of people who profit so much from its current dysfunction. Unless there is some sort of major disruption that completely changes the landscape (very unlikely), you can expect pharma in the US to be extremely expensive.
Look for ways to make the patents unenforceable. If diabetics had the ability to make their own safe insulin at home that would be best. Then all they would need is an internet connection and some basic components. The closer we get to that ideal the more empowered they are.
This would actually solve a lot of price gouging for drugs.
However that's only a stop gap measure. What's happening with gating access to insulin is happening to a thousand other products in a thousand other industries right now. Start looking at alternative governance structures. Lord knows everyones got a blog and a half-assed plan to run things better at this point (since the bar is so low).
Just don't poke the bear. As cathartic as hanging 'congresscritters' would be it wont actually solve the problem.
Basically act like you don't expect anyone else to fix this problem for you because nobody is going to; especially if you voted for them.
Price controls don't work. This is a solved problem and understood by nearly all economists. They lead to over/under production, huge waste, less efficiency and regulatory capture.
The question is why no one is calling for price controls for other products that are produced in a relatively free market. Then ask yourself whats different about the market for insulin that prevents price competition.
Using "fixed" prices to control costs is like using "fixed" thermostat readings to control global warming.
The way price controls are achieved for medicine in the first world is through negotiation between the state public Healthcare system and pharma companies. This actually, provably works, and has worked for decades, and is much more efficient than in the US in fact - both in terms of healthcare outcomes, and Healthcare costs.
I guess you have a lot more faith in "state public Healthcare system". Many comments were about how corrupt the politicians that led to this system were, so I imagine they would be equally as corrupt when they're "setting prices".
The alternative would be to allow people to break the third party payer system and allow people to buy and import drugs from whomever they want. You can do this now on the grey market, but it would be great if it were legalized. Then you can probably get it for the same price as any other country, probably even lower. If you want, you can have the state cut every insulin user a check for $10 a year or whatever it would cost in a free market
What I mean is that traditional avenues for change have been closed by the pharma industry lobby. It is not very different from the situation with the oil industry. The traditional political system has been corrupted by these industry forces, which support both parties.
Solving america’s problems with tech has a pretty good success rate. We tried addressing covid with social solutions (social distancing, self-quarantine, etc) and it was generally a complete failure in comparison to the technological solution (mrna vaccinations)
"African American adults are 60 percent more likely than non-Hispanic white adults to be diagnosed with diabetes by a physician."
Given that the middle class is very white and employed with insurance coverage, it virtually doesn't affect white people. Our politics takes black people's votes for granted and don't do anything for them.
>Our politics takes black people's votes for granted and don't do anything for them.
It's worse than that. If they sufficiently pandered to them to the point of actually solving their problems then they wouldn't be able to take those votes for granted, so they'll never solve their problems.
You're not wrong but the fact that the problem is allowed to persist certainly something to do with "people with enough spare f*ks to give to be politically active" being mostly unaffected by the problem.
IMO it's more helpful to look at this through an economic lenses than a race one. T2 diabetes is very much a poor person's disease.
There's people in at least one party who talk about problems like this, and given that party is the only one that has taken any kind of health care policy seriously for longer than the lifetime of this forum, and has at least some modest achievement to show for it during the narrow window they've had essential control of national institutions, there's reason to take that at face value.
And while various poll access restriction measures are an injustice one could almost think is intentionally targeted at black people, I imagine those obstacles aside they'd be as free and capable of conscientiously assigning their votes as anyone else.
Are you talking about the Democratic Party? They are more responsible for the extreme cost of healthcare in the US than any other political faction. Mandatory insurance, COBRA payouts… Did you know Gretchen Whitmer’s dad was the CEO of BlueCross?
I say this as a leftist: the Democratic Party is the party of the health industrial complex.
> They are more responsible for the extreme cost of healthcare in the US than any other political faction
I await the explanation of your model revealing the drivers of healthcare costs and connecting them to predominately Dem responsibility with baited breath, nigh weeping for hope of policy-capable leftists in the meanwhile.
> Mandatory insurance
You know that's how socialized insurance works at one level or another, right?
> COBRA payouts
Is this a mantra or a point?
> Did you know Gretchen Whitmer’s dad was the CEO of BlueCross?
This is definitely not a point.
> the party of the health industrial complex.
As long as we consider approach healthcare primarily as an industry, yeah, there's going to be industrial interests tangled up with it. Should we do it some other way? Maybe. In which party do you think that conversation is even possible?
The Democrats are the party who put massive amounts of effort into derailing the only viable candidate to argue for public healthcare.
Maybe you don’t care about keeping predatory insurance companies afloat with COBRA payouts, or forcing healthy people to pay tens of thousands of dollars to insurance companies, but plenty of people do.
Look. I appreciate passion for the topic. I absolutely care about this too. I probably spend waaaay more time than a layperson should reading about healthcare problems and policy. Like a lot of other people here on an engineering forum like this, I know the power of approaching things as their own kind of system.
And it kinda looks like you don't yet. That's something I've no doubt you could fix, but you'd have to want it. Maybe even enough to google the term "socialized insurance." Or understand that when healthy people pay into risk pools... that's what insurance is.
> The Democrats are the party who put massive amounts of effort into derailing the only viable candidate to argue for public healthcare.
Presumably you're talking about Sanders. I encourage you to talk to his office while he's not running about other people who are supportive and enthusiastic about public healthcare efforts. There are plenty. Arguably not enough: if they'd had few more Senators to get past Joe Lieberman in 2010, Medicare-for-all-who choose would have been a reality then. As it was the ACA was a mixed but significant policy victory.
Health insurance is a commercial industry. There is absolutely nothing socialized about it. The CEOs of these companies are getting paid tens of millions of dollars. They are INCs. They are not socialized in any way shape or form.
They do have regulatory capture, mostly given to them by the Democratic Party.
I can't tell whether you're saying "Health insurance in the US is a commercial industry right now" or "there's no such thing as health insurance that is not commercial."
The latter statement is not true. Medicare for all would be socialized insurance, as would any single payer plan. There are other kinds of socialized insurance you can find in other countries.
The former statement is mostly true with notable exceptions, so we'll assume that's what you mean. You may not be aware there is socialized insurance in the US, though: Medicare and other state programs (and again, the vast majority of Democratic officeholders supported expanding access to that to everyone in 2010 via what was called the "public option" at the time, unfortunately they needed every last D Senator and Lieberman held out). There are also some non-profit private insurers.
> these companies are getting paid tens of millions of dollars. They are INCs.
The money flowing through these companies is not the problem. Getting paid to provide valuable services is not a problem. Even if you had a magic wand that you could wave that made Bernie king and M4A a reality, you would still need to employ people to source revenue for the general insurance fund, provide good financial stewardship over it, manage relationships with competent providers, provide service to people like you and I, etc etc. You'd have to pay all those people. Like Medicare already has to (and hires private parties to help).
It's likely that entirely socializing insurance would cut down on overhead (and certainly on any profit taking), but the thing is... that's already been limited. By who? Well... these Democrats you're suggesting are somehow primarily responsible for nurturing insurers. Where did this happen? The Affordable Care Act required insurance companies to reveal how they spend consumer premiums, and spend 80% of those premiums on care and efforts to improve quality of care. What companies can take in operating expenses and profits is limited by law to 20%.
Did you know that? If you didn't, why are you so confidently holding forth on this topic? If you did, why are you insisting on repeating the line that Democrats don't care and in fact are responsible for increasing expenses and capture of revenue?
> They do have regulatory capture
They have representation and influence in a democratic system. Arguably too much? Yeah. What's your plan for that?
> mostly given to them by the Democratic Party.
Again, you're welcome to lay out your model of how the democrats are responsible. If it's really limited to "other people in the party thought they'd make a better candidate/President than Bernie", though, you might want to see if you can come up with something stronger. And while you're at it, maybe start to admit at least to yourself that maybe you have some more to learn about this topic.
> Again, you're welcome to lay out your model of how the democrats are responsible.
Simple, prior to the ACA I was able to cover my health expenses out of pocket. I’m healthy and literally went to the doctor 3 times in a decade. After being forced by the ACA to buy unneeded and unwanted health insurance, I ended up paying >10k /year for literally nothing.
I’ve since paid so much in health insurance that I could have covered my own cancer treatments, out of pocket. I have received nothing for that $100,000+ dollars.
Add to that the “marketplace” with limited time windows, limited competition, the inability to get insurance from another location…
These were all Democrat initiatives that I lived through.
Then, twice the Democratic Party fought tooth and nail to kill M4A. Biden literally said he would never implement it. I’m no fan of the GOP, but when it comes to healthcare costs, no one is worse than the Dems.
Insurance is not something you have because you are ill, it's something you have as a hedge against the probability that you will be ill. Whether you're healthy now has limited bearing on that.
And if you want to be able to have it when you are ill, you need to be willing to contribute to premiums even when you're not. Whether that contribution comes in the form of an explicit premium paid into a risk pool administered by private insurers or in the form of a percentage of your tax dollars paid to a socialized insurance plan (like M4A), that's how insurance works.
From a political standpoint, the individual mandate might have gone down more smoothly if people had been given a choice to opt out of it, in return for agreeing that they could be denied for pre-existing conditions. Democrats at the time made the calculation from a policy/values that too many people wouldn't understand what they were doing and end up shooting themselves in the foot. I used to think that was wrong.
> I ended up paying >10k /year for literally nothing.
> I could have covered my own cancer treatments, out of pocket. I have received nothing for that $100,000+ dollars.
Your numbers don't add up.
Out of pocket costs for a course of cancer treatment usually run well over $100k (and those stats might be for people who do have insurance).
There haven't been many years that the individual mandate was in effect. It went into effect in 2014. Tax for not buying insurance was lowered to zero by 2019. Your yearly premiums would have needed to be not ">$10k" but around $20k for you to have spent $100k in premiums.
And if you didn't want the insurance, it was always legal to simply pay that tax on not having it. How much? Well, for the median income household, that'd be about $700. Much less than You would need to be pulling something north of $500k a year in order for your tax to be $10k. Please, tell us where you worked, and why they were paying you that much while... not offering you insurance?
Or if you were making $500k a year as a business owner / contractor... why you didn't have any accountant or other financial professional giving you better advice? $10k a year in individual premiums is cadillac plan territory, even in expensive metro areas. Generally not what people who are healthy and go to the doctor three times in a decade buy. High-deductible plans with premiums below $300/mo are available to individuals in Los Angeles today. Your individual max required premium shouldn't be more than $3500 a year in 2021 (and in 2014, you could probably get away below $2400/year). Hell, you could cover a family of four in Los Angeles on less than $500/mo in premiums with ACA assistance, for a total cost topping out below $6000/year, so we know that's not what you're talking about (on top of the fact that you spoke in terms of your own health rather than mentioning any family).
Maybe there's some reasonable explanation for why all your numbers are so far outside of credibility here?
> the Democratic Party fought ... M4A
Please. M4A wouldn't even exist as a relevant concept in American political discourse without the Democratic Party. The only reason you know the label at all is because it was advocated in primary contests and by Democrats in congress. Yes, Democrats plural. For an example, read one piece of introduced legislation:
Notice the list of D Senators as co-sponsors. Notice that it is not short (nearly a third of the caucus at the time). It is profoundly wrong to characterize the Democratic Party as the primary obstacle to something like M4A when it is the only reason why M4A is a potential reality in the US. And saying "I'm no fan of the GOP" doesn't ameliorate that mistake: you can guarantee that the list of Senators sponsoring anything remotely like that bill in the GOP would have a length of 0 (and of course, given when the bill was introduced, only someone who was also ignorant of the composition of the senate at the time could think the primary reason it didn't go anywhere was D efforts).
Also, maybe check your misconceptions about Biden:
After I married a healthy partner: $2100 /month for the both of us.
After transitioning to full time employment: $2300 /month
These numbers align with my friends. In no way was paying $300 /month an option.
Health insurance is not health care. I don’t want it. I want public healthcare, barring that I want affordable healthcare. Pre-ACA was much more affordable.
I really wish neo-liberals could just admit when their policies fail. This one is not on the GOP. It’s 100% the result of DNC policy and actions.
I assume you want people to vote Democrat. To be effective there, step one would be to listen to people who have legitimate grievances and when your party is at fault, own it. Do not go on a tirade about how paying for insurance is actually a good thing. It’s not, it’s a failure of our social safety net.
I have no misconceptions about Biden. He was part of the admin that screwed me with the ACA, I watched every debate and heard him repeatedly state that he was going to continue to enrich the insurance industry on my back. Which is exactly what he’s done since taking office.
Spending and costs are distinct, of course, but they're related, and you'll see spending track costs directly unless there's a factor that increases/decreases demand for services
What do we see? An acceleration bump in 2014/2015, and then it settles back into data whose variation is much like pre-ACA dynamics. 2014 would have been when the exchanges and wide reach of access went into effect. The spending acceleration bump was almost certainly people who didn't have access before using medical services.
The idea that the ACA drove some kind of unprecedented increase in costs doesn't track:
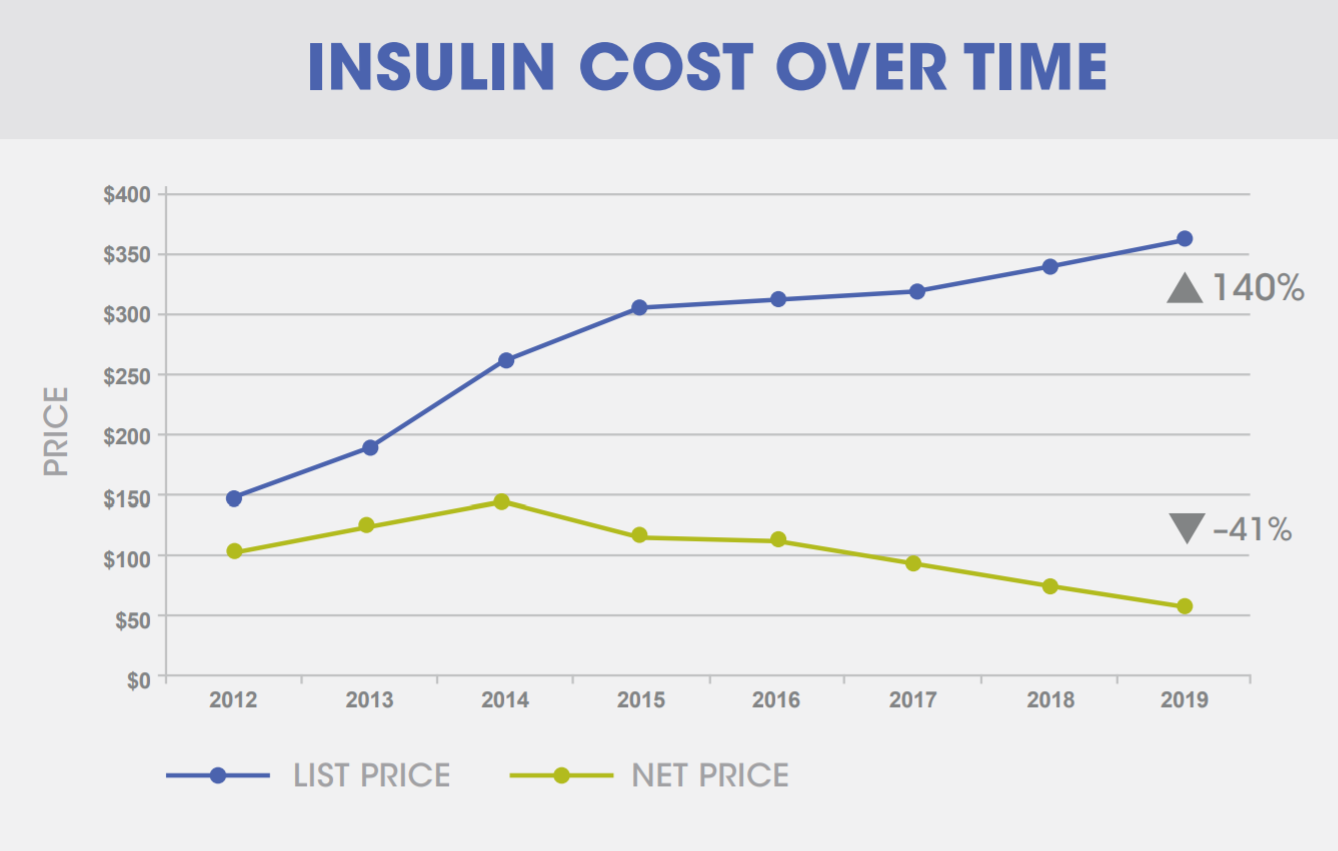{kind=link}
Could someone please point me in the right direction where I can read anything with more substance than a news article quoting an interview?
EDIT: Just to clarify. We're extremely fortunate that we're in Australia. Insulin is affordable/subsidised here, my daughter's CGM (and sensors) are free, and anything else we need is heavily subsidised too. I've no intention of biohacking anything to do with my daughter's Type 1.
I'm asking the above mostly because I'm curious. Admittedly I find it a bit scary that I know so little about the manufacturing of something that is 100% vital to my daughter's survival. I'd like to know more.