It's likely not what your doctor prescribed, it doesn't last as long, it requires you (or your young children) to eat on a very specific schedule, it can't be used with an insulin pen or insulin pump, it's just all around a worse and less effective treatment.
Seems like everything is working as intended? A corporation invests money to develop a better product, and the government gives them a 20 year monopoly on it so they charge a premium and recoup their investment. As a patient if you want to pay the premium for it, you can get the better product, otherwise you can still stick with whatever walmart's selling. It's worse, but it's not any worse than what you'd had if the company didn't come along and invented the better product.
That's not what is happening. It has nothing to do with a patent monopoly or recouping any investment:
FTA:
>In 1996, a vial of Humalog produced by Eli Lilly cost $21. Today, it's priced at $324 despite the cost of production remaining steady.
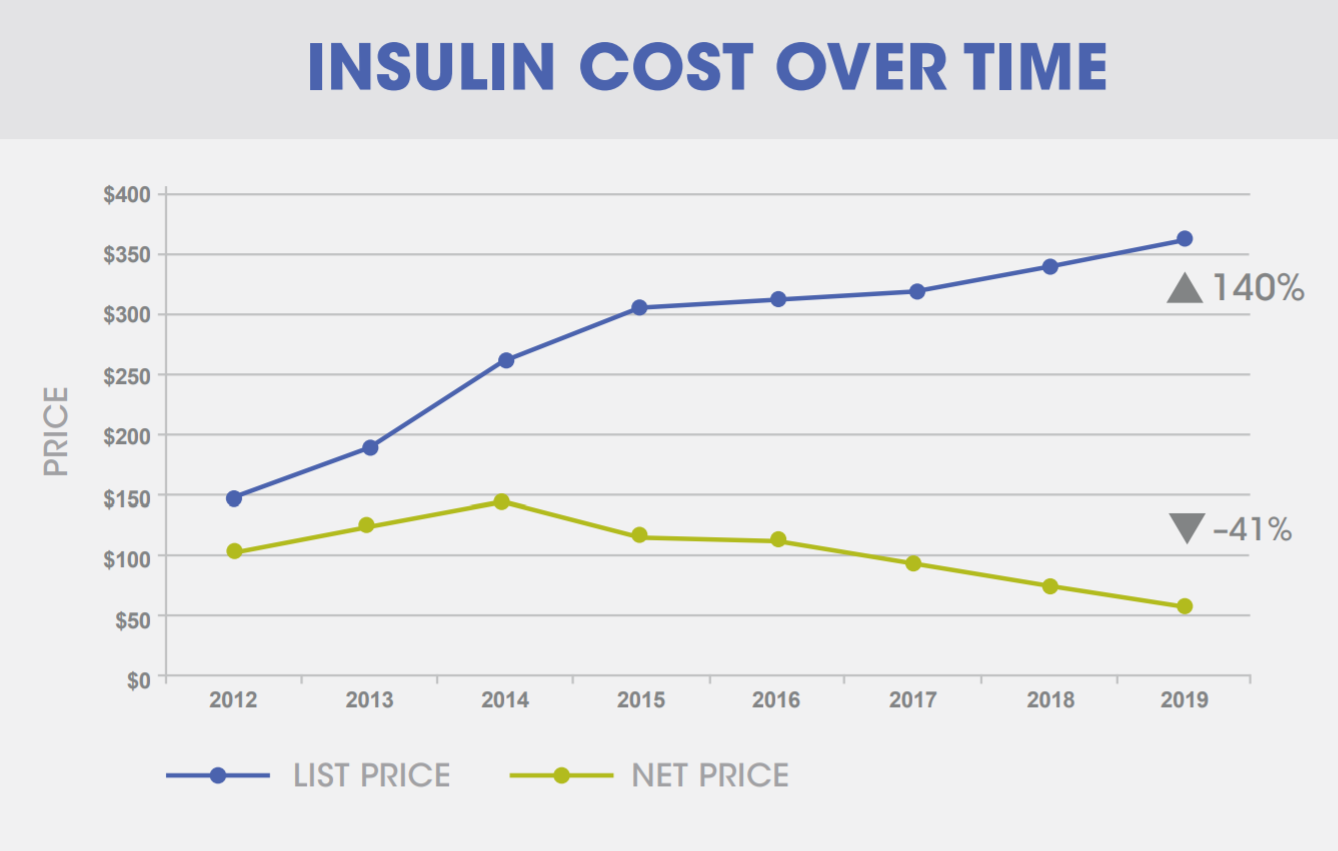
>Rising costs are nothing new. Insulin prices tripled from 2002 to 2013, and doubled between 2012 and 2016. To put this into perspective, in 1996 a vial of Humalog produced by Eli Lilly cost $21. Today, it's priced at $324 despite the cost of production remaining steady.
If everything is working as intended, it begs the question, what institution intended for patients to die from rationing insulin[0], and why is the USA ok with that institution's intention?
If it was developed in 1996, the patent protection would have expired by now. If the cost of production was "steady", then the question is why is a competitor not jumping in to make and sell something that would earn them a huge profit margin?
Do you doubt it was developed in 1996? Do you have evidence that the cost of production has significantly risen?
Otherwise, you seem to be repeating the old economics joke:
"The young economist looks down and sees a $20 bill on the street and says, “Hey, look a twenty-dollar bill!”
Without even looking, his older and wiser colleague replies, “Nonsense. If there had been a twenty-dollar lying on the street, someone would have already picked it up by now.”"
When there is a claim that there exists an arbitrage opportunity worth billions of dollars, I would consider it common sense to consider why has no one claimed the arbitrage opportunity yet.
The world has many very smart people spending many hours working very hard to find these opportunities, so the likelihood of it just sitting there like a $20 bill on the street, and not being picked up, seems quite small.
I do not know the answer myself, so I am interested in finding out. reddicky posted this:
>Biotech insulin is now the standard in the U.S., the authors say. Patents on the first synthetic insulin expired in 2014, but these newer forms are harder to copy, so the unpatented versions will go through a lengthy Food and Drug Administration approval process and cost more to make. When these insulins come on the market, they may cost just 20 to 40 percent less than the patented versions, Riggs and Greene write.
So it looks like there is some expensive expertise involved and investment into R&D that needs to be done.
Yes there is expertise and capital costs involved, which make it not an arbitrage play. It is more like a cartel, which seems to explain what is going on here, with the 3 insulin producing companies all fixing their prices together (at least in the US)
In theory there is 'nothing' stopping another company from coming along, even a group of Biohackers may try to do something - I wonder if that's been done... :)
The reason no one will pick it up is because there are massive capital investments to get something like that up and running, and the existing manufacturers can just drop their price to compete with you as soon as you get up and running. Now you have to recoup your capital costs in a saturated market, and your competitors can probably make insulin cheaper than you due to pre-existing economies of scale.
I would imagine that even other companies already in the pharma space would be interested. They don't want to play the race to the bottom game with billions of dollars in upfront costs. If anything, it's probably more profitable to make a new form of insulin that you get to patent. Which is how we end up where we are.
Although... I needed to buy a vial of the newest fast insulin in Spain last year without an insurance. One vial was 28 euros, which is much less than people in US have to pay.
The insulin in question is Lyumjev from Eli Lilly.
This is an incredibly stupid comment. Net price in Humalog has decreased since 2014 [0]. The PBMs jack up the list price so they can get their fat rebates.
Eli Lilly's profit margin is double digit, usually around 20%. Managed care organizations (insurance companies), which own the PBMs, have profit margins of ~5% or less.
That is a nonsense talking point from the industry. They use passthrough revenue to distort their profit margin. Express scripts is closer to 15% and CVS is closer to 10%.
If these PBMs are making lots of profits, then they are simply subsidizing losses elsewhere in the MCO. The total costs paid for insurance premium plus out of pocket costs by the end user in the US would not be affected.
You are not addressing my main point which is that these MCO's distort their "net margin" stat using accounting tricks. And yes PBM's are INCREDIBLY profitable. Express scripts made 4.5 billion in net income in 2017. They have never produced a drug that has saved a life.
PBMs are important but they should not be able to put a gun to these pharma companies heads because they control the formulary.
CVS net margin includes their retail business. You can't compare AWS's margin to Walmart's e-commerce margin.
I am not addressing it, because I do not see any further evidence of distortion of an MCO's net profit margin other than what this article claims. Nor would it matter to me unless some MCO executives are smuggling cash out of the country or something.
As a customer, it does not affect me.
In the healthcare business, the flow of money is:
Individual -> MCO (insurance company) -> healthcare providers and drug manufacturers
What does it matter to the individual what portion of an MCO is earning what profit if the net profit margin of the whole MCO is 5% or less? They are obviously not left with a lot of money, their employees are not known to be lavishly compensated.
That doesn't seem too strange when you consider that those two types of companies have different operating models. A drug company is in the business of taking relatively cheap goods and converting them to very expensive goods, in other words adding a lot of value. A insurance company/PBM is mostly in the business of skimming a percentage off transactions.
It is not strange, but it also contradicts claims about managed care organizations earning tons of money. It is not a business you go into to get super rich.
Yes it is working as intended, the argument is that those intentions are inhumane. Can you think of any medical treatments that were developed without the promise of 20 years of limitless profits? I can.
> Can you think of any medical treatments that were developed without the promise of 20 years of limitless profits? I can.
This sounds like it's responding to a strawman. Proponents of the patent system aren't claiming that zero innovation would happen without patents, just that it would be much less. In other words:
No patent system: only inventions from altruistic inventors
Patent system: inventions from altruistic inventors and profit-focused inventors.
Let's say corporations were only promised a 10 year monopoly instead of 20. Do you think their business would collapse, or would they keep trying? If profit-focused inventors could still be motivated by a 10 year horizon, then that extra 10 years only benefits corporate executives and kills patients. So, is the patent system as limited as possible while still encouraging innovation? Obviously not, because pharma companies routinely direct billions of dollars in profit into stock buybacks instead of research or any other actual investment. They can easily afford to make less profit.
It would depend on the project's margins and/or sunk costs. A project that had very little invested in it or is a breakout success might we able to weather a 50% cut in exclusivity period, but a marginal product might not. Most of the already developed drugs are probably going to be fine, assuming that the financing for them was already secured.
>or would they keep trying?
For the projects at the margins? most certainly. That is not to say all private drug development would, stop. If some sort of unpatented-but-super-cheap-to-perfect-but-still-not-patented drug showed up it might still be developed, but in aggregate I'd expect drug development to drop significantly.
I am arguing that there are no marginal projects at current profit levels, and that's why they can spend billions on stock buybacks. There is a point that lessening patent protections would cause companies to cut back, but we are not at that point.
Define fair and unfair. If it was so "unfairly" lucrative, I would have to ask why everyone does not invest in pharma? Why are tech companies where much of the VC funds land?
Perhaps it is because there a huge amount of risk involved?
{kind=link}
It's likely not what your doctor prescribed, it doesn't last as long, it requires you (or your young children) to eat on a very specific schedule, it can't be used with an insulin pen or insulin pump, it's just all around a worse and less effective treatment.