> Whereas lockdowns in the Covid-19 case might have contributed to a lengthening of the crisis by delaying herd immunity
The point of the lockdown was not to entirely stop the spread- that was obviously not happening. It was to slow the spread to avoid overwhelming hospitals.
It allowed us to reduce the lethality of COVID-19 by having more resources per sick person.
I assume experts look at a large number of factors to assess whether it should or should not happen and measure the disease by a variety of metrics.
Also I'd assume the urbanization, science, and ability to execute a lockdown changes over 62 years. Also the nature of work is different. Nobody was doing home computer video conferencing in 1958.
If anyone really wanted to compare it, they'd probably need to have some technical expertise in both diseases and also be some kind of specialized historian.
Expected deaths from an unchecked epidemic: 330 million × 50% infection rate × 4% fatality rate = 6.6 million.
50% infection rate is the estimated no-lockdown epidemic penetration rate that I remember hearing from an epidemiologist. 4% was the fatality rate in Italy, February 2020, when hospitals were overwhelmed.
Did you actually look at the population pyramid for Italy, and compared it to the one for the US, before you made that argument? I don't think you did.
Besides, even if the true number was 3.8% or 4.3%, that wouldn't change the conclusion.
First: we do not know that the lethality would have been without lockdowns. We didn't (often) see hospitals turning people away. The lockdowns succeeded in preventing that.
But more importantly, it's not fair to judge people based on the decisions they made in the past with the information they had then, using the information we have now.
Let's presume there was no difference in lethality. We did not know that at the time. But it was reasonable to believe it would be helpful and save lives.
Who is sitting there going "yeah but what if it doesn't save any more lives? Let's risk it because I've got a party planned next weekend".
I was in my wonderful homeland of Bulgaria. Every time a person died, the hospital always wrote down Covid, so they can get extra money from EU and the state. Car crash? Covid! Old age? Covid! AIDS? Covid! Drank bleach? Covid! F***ing Bulgarians living in year 3020.
We had people saying the same thing where i am in the states. Except that county mwdical examiner records are freely available online and did not reflect that in any way shape or form.
There were still, far more deaths from overdose and suicide than Complications of Covid-19.
That's like rebutting complaints of a rigged election by saying "the vote results for each county are freely available online, and look, clearly candidate A's votes add up to 51%!".
The original complaint is that hospitals were (and provably so?) given instructions on how to mark Covid deaths for statistical purposes, and those instructions were biased to inflate the numbers. At the time this was labelled as a "conspiracy theory" in order to drive the narrative, and afterwards it came to light.
"Medical examiner records" can't prove this, because they might as well have been doctored. No non-stupid person would write a report talking about patient having serious conditions A, B, and C, and then fill in a field for "cause of death" with "Covid", so of course you won't find any examples of that.
Let's all be honest, the media got caught with their pants down driving a narrative to fit what they felt was right and what "TPTB" wanted, and we're all in denial now about it. The truth will eventually come out.
With there being no evidence of this supposedly widespread doctoring of records, sounds more like right-wingers got caught with their pants down driving a narrative to fit what and what they felt was right and what "TPTB" wanted, and you're all in denial now about it. The truth is out.
My general opinion of it is that lock downs at the beginning were essential for slowing the spread of the disease and allow the hospitals to prepare for it, but there was a point where the virus was endemic anyway that all the masking and isolation protocols were doing more harm than good.
They were doing it even before covid, although not to the same extent. I don't know why people have such a problem if someone wants to protect themselves from airborne illness.
If someone harassed you or a loved one for wearing a mask, that person is an asshole. If someone harassed you or a loved one for not wearing a mask, that person is also an asshole (caveat outside hospitals or care homes for vulnerable people).
One of the largest peer-reviewed European studies says...
"These findings indicate that countries with high levels of mask compliance did not perform better than those with low mask usage."
https://www.cureus.com/articles/93826-correlation-between-ma...
Why? Because they are ineffective and were only introduced as a way to busy or "pacify" the masses.
I believe that is what pre-COVID masking in hospital settings has shown, yes. Possibly COVID is different from the flu.
But the difficulty for proving masking helps is:
1. If it only takes ~20 virions to get infected, then masking has to have a basically perfect filtering rate and be worn perfectly 100% of the time, neither of which is obvious.
2. With an endemic virus even if masks slow down spread they aren't going to reduce your likelihood of being infected overall.
> Consistent use of a face mask or respirator in indoor public settings was associated with lower odds of a positive SARS-CoV-2 test result (adjusted odds ratio = 0.44). Use of respirators with higher filtration capacity was associated with the most protection, compared with no mask use.
I'll take a reduced risk, even if it's not perfect. Would you prefer to get covid one time, or five times? It's like arguing "why bother wearing a seatbelt, when it doesn't prevent injuries in accidents?"
Also, are you suggesting masking does not help with preventing influenza infection?
How did they account for people "doing something different" when wearing a mask? I.e. did they do a double-blind experiment where people wore masks that had intentional holes in them? So we can know that wearing a mask is the thing to do vs whatever it is that wearing a mask caused that person to do. I guess I'm asking or saying that this might have been some sort of "correlation is not causation" kind of thing?
I get that for whatever reason folks like yourself don't want to believe it, but trust me, masks work. Just ask anyone who works in asbestos abatement or BSL-2+ facilities.
Yeah but there were and are nasty side effects to this, covering literally hundreds of millions or rather billions of people in some form. Missed social interaction is super important for child development, but how do you want to measure that, how many harm points do you assign to this versus some old or frail person dying. And look at ie India, delaying the height of infection didn't help them at all, estimated numbers of dead there are what, 5 millions? Let's not focus on just few wealthy nations, human life is human life regardless of origin.
Also psychical stress from prolonged withdrawal from most if not all social interactions. We fucked up economy pretty badly and still seeing the results of it, made millions of financially very vulnerable people lose their job or family business overnight. And so on and on. Typical HN crowd is probably the least impacted so we are not a good sample to discuss this objectively.
In number of deaths alone yes it was without question the best course of action. The bigger picture, I am not so sure. And cases like Sweden show that restrictions were mostly stupid flexing of control powers by politicians who were generally during crisis clueless as fuck, and the harder they went the more they polarized non-trivial part of society. Again we still see the effects and they are not going anywhere, ever.
If I would be and old and frail person in high risk category, I personally would take all effin' risks and don't screw up childhood (and conversely rest of life) of my grandkids. But that's just me.
> And cases like Sweden show that restrictions were mostly stupid flexing of control powers
I wish this meme would die. Not only did Sweden not do well in the pandemic, they also ended up enacting a ton of restrictions, some more stringent than what much of the US had in practice.
Between the unprecedented amount of money that was injected into the economy, the PPP loans, and the low interest rates, we’ve seen one of the largest transfers of wealth ever. The coming inflation will certainly cement the growing class divide. Hopefully nobody reading this is poor because the reality is that you’re most likely going to continue being poor throughout your lifetime, and you’ll probably become much poorer relatively compared to those who were able to capitalize on COVID policies.
It also was to increase the number of people who got covid after being vaccinated, instead of before.
Edit - to elaborate, I just mean that it made sense to try to keep infections down and give companies time to develop a vaccine. Not sure why this struck a nerve.
I think you got downvotes because it sounded like a conspiracy theory, when actually I think you were just trying to say that the idea was to get people vaccinated before they came in contact with the real disease to ease the symptoms, or even give immunity.
> So the vaccines did not prevent infection nor transmission.
Yeah they did. They just didn't do it perfectly. And only about half the people out there got vaccinated. So vaccines failed to be a silver bullet that ended the pandemic.
Can you name a single vaccine that prevents infection and transmission, as in "nobody with the vaccine gets sick or gets someone else sick"? I don't think such a vaccine exists, but I might be wrong.
CDC says Polio is "99 - 100 % effective" against paralytic polio [0]. So essentially perfect efficacy. Covid vaccines look like a failure in comparison (<60% effective against hospitalization, much more significant harms)[1]
To me the problem wasn't that the vaccines didn't perfectly to prevent infection and transmission; the problem is that the messaging from the medical field was that the vaccine _would_ prevent transmission and harmful reactions would be rare. No matter how much one squints, neither of those look remotely true.
> CDC says Polio is "99 - 100 % effective" against paralytic polio [0]. So essentially perfect efficacy. Covid vaccines look like a failure in comparison (<60% effective against hospitalization, much more significant harms)[1]
You're using an arbitrary delineation which the parent didn't. "Essentially perfect" is imperfect, just like the Covid vaccines - because the measure wasn't "more than 99% effective", it's "100% effective".
> To me the problem wasn't that the vaccines didn't perfectly to prevent infection and transmission; the problem is that the messaging from the medical field was that the vaccine _would_ prevent transmission and harmful reactions would be rare. No matter how much one squints, neither of those look remotely true.
When and by who was this messaging put out? The Covid vaccines are pretty darn good at protecting you - but only from the original strains, they're not good at protecting from mutated strains. You need updated shots for that, by which time the virus has mutated further.
I’m not implying that the numbers I choose are the best to use, but I think they are a fair indication of a vaccine that is very effective vs one that is marginally effective. If you have some numbers that are less arbitrary, I’m open to new info to change my mind.
During the pandemic most health institutions were being really optimistic in their messaging about the vaccines. I guess it’s just semantics, but I don’t think you can say a vaccine is darn good then say the virus mutates too fast for the vaccine to be effective long-term. Aren’t those things in opposition?
> I’m not implying that the numbers I choose are the best to use, but I think they are a fair indication of a vaccine that is very effective vs one that is marginally effective. If you have some numbers that are less arbitrary, I’m open to new info to change my mind.
I don't think that any specific number is a good delineation between "ineffective" and "effective". I fundamentally disagree that the Covid vaccines are ineffective. The only way to call them ineffective is to use a delineation which no vaccine survives.
> During the pandemic most health institutions were being really optimistic in their messaging about the vaccines. I guess it’s just semantics, but I don’t think you can say a vaccine is darn good then say the virus mutates too fast for the vaccine to be effective long-term. Aren’t those things in opposition?
No, they are not in opposition. You left out the important part: the vaccines are darn good against the original virus. They are still sorta good for mutations.
Without a delineation, how do you argue that it is effective? How how do you argue that any treatment is effective if not statistics like these? And it’s not fair to say no vaccine survives this delineation because I specifically used Polio as an example of an effective vaccine.
There isn't a magical number which means the vaccine is effective, and below that number it is ineffective. A vaccine is effective if it helps people deal with a virus (i.e. lowering chance of hospitalisation/death). It doesn't magically become ineffective because it doesn't meet an arbitrary percentage of prevented cases.
The Polio vaccine is "only" 99-100% effective. That means that it's not 100% effective (as in, there are cases where it doesn't prevent transmission/infection). According to the criterium laid out by GP this means it is an ineffective vaccine, just like the Covid vaccine.
But they don't prevent infection nor transmission. What is the word to describe a proposed medical treatment that does not work?
Both the Covid vaccine and the vaccines you are saying had great results share this trait. You mentioned this negatively for the Covid vaccines. Why is it different for other ones?
I don't know anyone, in western countries, who got polio vaccines and suffered illness. I know people who took the covid shots and boosters and got sick with covid and variants. Some got it multiple times, so somehow the covid shots are interferring with sterilizing immunity.
> Some got it multiple times, so somehow the covid shots are interferring with sterilizing immunity.
How do you get to this conclusion? People without vaccination seem to be more likely to be re-infected. If anything, Covid itself is interfering with sterilizing immunity, and the vaccines help!
That is simply not how the vaccine was presented by authorities and the media. They literally said the vaccine will stop you from getting it and stop transmission. It took them months to acknowledge you could still get it and spread it with the vaccine and all the data simply points to a reduction in severity of symptoms.
What happened was they rolled out the vaccine before they had all the data, and it was bit oversold despite lack of data, perhaps to encourage people to get it.
It's water under the bridge now. But don't gaslight people on what they were told.
They were lying. Or at the very least didn't understand the claims actually made by Pfizer/etc, which was only that these vaccines prevented the disease, not that they prevented infection/transmission. They made no claims about infection/transmission.
It comes down to the stupid conflation of SARS-CoV-2 and COVID-19 into just "covid". Pfizer/etc use the two terms correctly, saying they prevented COVID-19, but didn't say anything about stopping SARS-CoV-2, but because everyone thinks "covid" is the virus they can't seem to understand what was actually said.
No, it's true. The matter of fact was that some collective hypnosis or lie was happening, and when you told people that the vaccine wasn't meant to stop transmission, they would just get angry from the cognitive dissonance.
No, we, who are rational truth-seekers, are the ones who were gaslit for 2+ years about the whole idea of "natural immunity". Despite having had covid and recovered from it, we were still told we needed to vaccinate even AFTER recovering from it.
It wasn’t even entirely that, although it certainly was in the seattle area at the beginning and in New York when refrigerated trucks were filling up fast. It was to “flatten the curve,” which was to allow for effective treatments and buy time for vaccine development.
Unlike in the 1950’s, we knew early on we could produce an effective vaccine. The vaccines that were eventually developed were designed within weeks of the viral genome being sequenced.
However we also didn’t know how to stop people from dying from covid at the beginning. It took some time discover pronation and other treatments that’s improved mortality.
Finally I would note that the articles celebration of a five times worse outcome as some sort of victory is survivor bias at its worse. “See, everyone who didn’t die didn’t die!”
I think there will be plenty of review of what was effective and wasn’t. Maybe lockdowns lasted too long. Maybe they didn’t. But this article is less than convincing.
Their metrics are also off. In 1959 the US had a population of 159m. In 2020 it has a population of 331m, a 208% increase. However in the pandemic 1.14m Americans died. They quote 0.119m deaths. How they come to the conclusion of “with a broader reach for severe outcomes than Covid-19 of 2020,” it’s hard to tell.
I'm not seeing that we knew anything. I'm seeing that a lot of work had been done to create a potential for success. Can you point out where this "knowing" is coming from in the linked paper?
In real life there is no certainty when faced with a new thing in nature. But there were many concurrent potentials for success - including traditional vaccines like coronavac. But it’s important to note that human trials for mRNA started in March, a mere two months after the genome was released. As we know now the antibody response to mRNA vaccines are rapid and robust. This information didn’t reach us immediately, but it reached public health decision makers world wide. Inactive vaccine trials started in April, a mere month later, and had good response if not as great as mRNA. Likewise monoclonal antibodies were approved in April as well, and pronation was proven and publicized in April, along with other treatments and techniques. So, as a decision maker, “flattening the curve” seems like a great strategy given you have rapid progress on multiple fronts. In 1959 absolutely zero of these were possible or probable. Monoclonal antibodies were perfected just 40 years ago, pronation wasn’t widely recognized as a possible treatment, and mRNA wasn’t even science fiction. The article proposes an absurd calculus from two completely different worlds as if they were somehow identical decision making criteria. It wasn’t, and while there was no “knowing” any one of the avenues would world, it was almost certain one would - especially with so much research behind the safety and efficacy of mRNA presented in my linked article and the remarkable and robust antibody response in the first humans in March.
This is an interesting read… one of the challenges of the revisionism in articles like the original link is they simply ignore all context and lie about any context they include (deaths per capita being more extreme in 1959 etc). Besides being viral outbreaks almost nothing of the context is similar. That’s why people say in the thread this is an anti science article - a huge amount of the decision making context was the state of science and how amazing it is in 2020 vs any other time in all of humanity.
>The point of the lockdown was not to entirely stop the spread...
That claim is pretty inconsistent with the marketing slogans and messaging about the purpose of the lockdowns.
Similarly, the vaccines turned out to be ineffective for inducing sterilizing immunity, but good for diminishing the severity of symptoms, which would also result in fewer sick people in hospitals. But again, the marketing and messaging around the purpose and intent was completely incongruent with the reality, seemingly intentionally deceptive at times. If you didn't take the vaccine, you were literally killing and holding everyone else back because the vaccine would ostensibly make you immune and prevent the spread.
The biggest failure of Covid was the disingenuous communication.
VoodooJuJu says "The biggest failure of Covid was the disingenuous communication."
"Disengenuous communication" is a vague term. I think rather that the biggest failure in the USA was for the government to intercede at all and to adopt protocols that delayed immediate treatment. By delay of treatment I mean that the protocol doctors were instructed (and later forced to use) was:
1. Tell the patient to stay at home (do NOT visit the doctors' offices) until (s)he can barely breathe and to then
2. Go to the hospital where they can hook you up to a ventilator and where you will die,
Rather than
3. immediately prescribe hydroxychloroquine (or ivermectin, or other...) and antibiotics (to prevent secondary infection, not the Covid virus) for home use, and go to the hospital only if it gets significantly worse.
Countries who jumped immediately to 3 had far fewer fatalities (indeed, far fewer hospitalizations) than the USA, who followed the steps 1-2 (and omitted 3 or did 3 in a hospital setting far too late to work), above. Consequently the USA suffered extremely high Covid deaths:
Even worse, it appears that the USA "powers that be" did that to justify established institutions and corporations who stood to make billions of dollars creating not-yet-existent (and later incompletely tested) vaccines instead of providing cheap and effective treatments that were readily available and that worked.
that is just total word salad. Please look up what habeas corpus means. It's right there in wikipedia or any other reference work of your choice. Informed consent is not a right. Those are enumerated also in reference works. Medicine in the united states is essentially the opposite of socialized. Good lord.
> Simply saying "you're wrong" is not an argument.
Right, which is why I followed up with a categorical and complete description of the problems with your nonsensical word salad.
>> Please look up what habeas corpus means.
> You cannot detain people without charges or probable cause.
No, you're thinking of the Fourth Amendment. Habeas corpus is the mechanism by which a person can report a suspected unlawful detention or imprisonment to a court, which can then order that the person be brought forward in person, in order to ascertain whether or not the particular imprisoning entity has the authority to do so. Obviously this has nothing at all to do with vaccines except in the fever swamps.
>> Informed consent is not a right. Those are enumerated also in reference works.
> > Medicine in the united states is essentially the opposite of socialized.
> And yet it was public health officials who imposed lock-downs. There is clearly socialized medicine in the US.
What you're referring to as 'socialized' here is the government, which we as citizens and resident aliens agree to recognize in order to increase and defend the common good. For example, we agree to being policed, we agree to being taxed, we agree to being bound by laws, and we agree in particular in this case to working together to try to stop the collapse of healthcare systems, even if that is inimical to the political chances of the president at the time.
> Right, which is why I followed up with a categorical and complete description of the problems with your nonsensical word salad.
Just because you disagree doesn't mean you have to be provocative and impolite. It's also against HN's rules BTW.
> Habeas corpus is the mechanism by which a person can report a suspected unlawful detention or imprisonment to a court,
You're making a distinction without making a difference. People were detained without charges or probable cause and were not allowed legal remedy.
> Obviously this has nothing at all to do with vaccines except in the fever swamps.
I was talking about lockdowns...
> Not therefore a right, got it.
Just repeating a statement won't make it true, it just makes you arrogant.
Informed consent directly derives from the right to bodily autonomy. It is such a basic right that if its blatant violation can be prosecuted regardless of jurisdiction. It is also protected by the 4h Amendment.
> What you're referring to as 'socialized' here is the government, which we as citizens and resident aliens agree to recognize in order to increase and defend the common good. For example, we agree to being policed, we agree to being taxed, we agree to being bound by laws, and we agree in particular in this case to working together to try to stop the collapse of healthcare systems, even if that is inimical to the political chances of the president at the time.
Actually "we" didn't "agree", what ever that means. The "common good" was never the foundation of the US, it was a Republic (thus power by and for the people) with limitations to protect individual liberties to limit the tyranny of the majority (the funding fathers were actually very critical of Athenian democracy BTW).
Taxes and police have their legitimacy through elected officials. But lockdowns and forced vaccination were put into place through edicts, the vast majority of whom were struck down by the Supreme Court, and thus never had the consent of the people nor respected individual rights.
No, but an infectious disease is also limiting on people's freedoms, so it's equally not obvious that those rights override the rights of people to be protected from infectious diseases.
Fundamentally, morally speaking those those aren't facts but opinions. Legally, I think it differs from country to country. Individual rights versus the needs of the state is something that we have really changed perspective on in the last hundred years.
There is no right to protection from infectious disease. It appears nowhere in the US Constitution. There was never any valid moral or legal justification for restricting the 1st Amendment right of freedom of assembly during the pandemic.
Well, that is not quite true at the State level. There are a number of States who have implemented laws that punish transmission of HIV/STDs knowingly. I'll concede there doesn't exist anything at the Federal level that I am aware of.
I would note that while the US Constitution is a valid authority with regard to legal justification (in the US!), it is very much not with regard to moral justification.
So at least in the US the founding political ideology is based on natural rights and social contract theory. Your conception is closer to patriarchal rights, which is in conflict (at least here in the US).
Well, it's not an absolute right (and it's obviously constrained by the limits of what it is even in our power to control). But then neither is the right not to be detained, or really any other right. All rights run into limits when they come into conflict with other rights.
I think it was a witness test of people's moral philosophy. Rights are fundamentally philosophical position, not a law of physics.
Those that favor preserving negative rights over positive rights generally objected to the lockdown.
In general, people who favor negative rights do so because they don't come into conflict with each other. Positive rights come into conflict with other positive rights and negative rights, and require trade-offs
I agree. My personal perspective is that I fundamentally don't agree that negative rights don't conflict with each other, or that there is a meaningful difference between positive and negative rights (which is of course a philosophical position that not everybody will agree with).
Negative rights not conflicting with each other is the main and perhaps only factor that distinguishes them from positive rights, so if you don't think that is true, of course you won't find a difference.
When it comes to practical implementation, the tools used to maintain negative rights are the same as the tools used to maintain positive rights, so they appear very similar.
If you're familiar with the concept, you probably already know that negative rights prohibit other people from actions, while positive rights require other people to take actions.
I'm curious why you think this distinction is not valid.
(2) The right to private personal space free of other people
On the face of things, neither of these require anybody to take actions. Nevertheless, one cannot fully exercise (1) without violating (2) and vice versa.
Interesting I think that is a great example of why and how the concept of personal property (bodily or material) is necessary to make negative rights consistent.
Also, the first right seems more like a positive right guaranteeing an entitlement to do or have access to something.
People are free to stay inside if they're afraid of getting sick.
Rights can only be overridden if and only if there are no other choices, which is not the case here.
Me getting to an hospital doesn't limit someone else's freedom.
Thousands of people going to the hospital at the same time due to a preventable phenomenon certainly limits the freedom of lots of people to continue living when those hospitals are overrun and unable to provide care. We had already tried a few months of the "let everyone decide individually and hope for the best" approach and the problem kept worsening superlinearly.
> People are free to stay inside if they're afraid of getting sick
By that logic, people are free to stay inside if I'm standing outside their door with a gun and they don't want to be shot. Yes, they're free to stay inside, but they're not free to go outside.
I think it's reasonable to believe that the rights of free movement override the rights to be protected from diseases in this case, but I don't think you can argue that via a general principle of rights. I think you have to argue that based on the specific consequences, and on your personal values.
Except the hospitals really couldn't do anything to help these people anyway and in some cases actually sped up their death with use of ventilators. Even more frustrating, they could have been giving things like monoclonal antibodies right away but they didn't.
Additionally, hospitals had years to figure out a better way of expanding their ICU's for emergency use. They also tend to operate on lowest required beds to save costs and began to quickly get overwhelmed due to their unpreparedness.
"It allowed us to reduce the lethality of COVID-19 by having more resources per sick person. "
This is false and there's no data backing this claim up.
> in some cases actually sped up their death with use of ventilators
The ventilator argument is brought up a lot so I wanted to share an article going over the related evidence:
"Based on the evidence at hand, we can reasonably say that there probably wasn’t a large impact either way from early intubation treatment paradigms."[1]
> Except the hospitals really couldn't do anything to help these people anyway and in some cases actually sped up their death with use of ventilators. Even more frustrating, they could have been giving things like monoclonal antibodies right away but they didn't.
Uninformed and wrong. ICU staff worked through extreme conditions to save many. Ask a few how much better their patients would have fared at home instead.
> Additionally, hospitals had years to figure out a better way of expanding their ICU's for emergency use. They also tend to operate on lowest required beds to save costs and began to quickly get overwhelmed due to their unpreparedness.
Expanding ICUs is not a matter of furnishing rooms, it's a matter of finding people with the requisite skills and experience. A localized need can be met by moving people around, but when every hospital in the country needs to grow its staff there is no way to conjure up more of this sort of person.
Statistical proof please. I don't care about your anecdotal evidence, especially when it was used for authoritarian lockdown measures that resulted in things just as bad or WORSE than what COVID caused.
For the mathematically-minded, it is worth noting that the Asian flu had an R naught of 1.7 while Covid had an R naught of a bit more than 2.
Keeping in mind these are fat-tailed distributions. So an R naught of 2 is a estimate of a true R naught, and because using sample averages to estimate means (true R naught is a mean) is unstable (the fatter the tail, the less moments of the distribution there are), once the reported number starts getting upwards of 2, the less confidence you can have that that reported number represents the true R naught. You have know idea if the superspreaders are infecting 50 or 500 people.
At the beginning of the pandemic, we were seeing R naughts estimates at 2.5. That's shockingly high. People were right to take extreme members in the face of that kind of uncertainty.
These people enforcing their values with 20-20 hindsight when the decisions were made given limited data at the time are causing harm to our collective ability to make decisions in emergencies.
For those that are interest in the nuances of modelling infections, I'm going to leave a Wikipedia extract here.
"R_{0} is not a biological constant for a pathogen as it is also affected by other factors such as environmental conditions and the behaviour of the infected population.
R_{0} values are usually estimated from mathematical models, and the estimated values are dependent on the model used and values of other parameters. Thus values given in the literature only make sense in the given context and it is recommended not to use obsolete values or compare values based on different models.
R_{0} does not by itself give an estimate of how fast an infection spreads in the population".
> it is recommended not to ... compare values based on different models
i.e. R0 numbers are worthless. You can't compare these values between pathogens, you can't even compare them between different academic groups studying the same pathogen or between outbreaks of the same pathogen as modeled by different versions of the same software. There's no agreed way to measure this value empirically.
Instead they write a program to simulate the spread of a virus through population and then (in effect) brute force one or more of the inputs until the results of the simulation match what happened so far. These variables are often given names that sorta reflect an intuition about what they're supposed to do, but they're just names. The actual values are arbitrary and there's no effort to ensure the computed values connect to the names in any plausible way.
A funny example of this was a COVID model from University College London that used household size as a free variable. The model used this value to achieve curve fit for each country in the study, so they reported that the average Brit lives with seven other people (the paper has 73 citations).
More seriously, estimates of R0 for SARS-CoV-2 have ranged from 1.5 to nearly 6, maybe even higher. It's not even clear what the definition is because it's not time bounded in any way. So not a value that's really knowable, like the speed of light is.
It would be useful to be able to measure some sort of inherent infectiousness, but R0 as actually defined and computed today is useless. It looks scientific on the surface but everyone who calculates it gets a totally different result, and because there's no actual underlying theory involved (just playing with stats), there's no way to decide which estimate is correct.
To get meaningfully constant values for infectiousness you'd probably need a microbiological / genetic theory that let you derive it from RNA sequences.
> To get meaningfully constant values for infectiousness you'd probably need a theory that let you derive it from RNA sequences.
As others have already noted in this thread, the rate at which a disease spreads inherently depends on both the biology of the pathogen and human behavior. For example, if everyone goes to crowded nightclubs, then R0 for an airborne respiratory disease goes up. If everyone stays home, then it goes down. The biology of the pathogen and human behavior interact in complex, multidimensional ways; promoting condoms will reduce R0 for HIV, but not for influenza. The disease spreads only through human behavior, so the concept of infectiousness independent of that simply doesn't exist.
You are correct that R0 is determined by curve-fitting to actual case counts. It couldn't be otherwise though, since that's the only way to capture the actual human behavior. We expect different R0 in different situations, so the range you see for SARS-CoV-2 isn't a surprise. This is textbook stuff:
> Any factor having the potential to influence the contact rate, including population density (e.g., rural vs. urban), social organization (e.g., integrated vs. segregated), and seasonality (e.g., wet vs. rainy season for vectorborne infections), will ultimately affect R0. Because R0 is a function of the effective contact rate, the value of R0 is a function of human social behavior and organization, as well as the innate biological characteristics of particular pathogens. More than 20 different R0 values (range 5.4–18) were reported for measles in a variety of study areas and periods (22), and a review in 2017 identified feasible measles R0 values of 3.7–203.3 (23). This wide range highlights the potential variability in the value of R0 for an infectious disease event on the basis of local sociobehavioral and environmental circumstances.
As with your confused understanding of PCR specificity, you may have been misinformed by indefensibly oversimplified public messaging as to the definition of R0. (I had a comment deleted from /r/coronavirus in 2020, because they considered my statement that R0 varies with environment and human behavior to be misinformation; the citation didn't help.) The literature is once again available for anyone who wishes to read it, though.
No, I'm not confused about any of this. I'm giving the textbook definition in this thread, right? I'm sure even sure why you are arguing with me instead of the user who started the thread by giving specific R0 numbers for influenza and SARS-CoV-2. As you say, you can't do that because R0s are characteristics of outbreaks, not viruses.
So the confusion is the other way around. An outsider to the field would think R0 would be defined biologically given it's called the "basic reproduction number" and because epidemiologists themselves regularly make claims like "influenza has an R0 of this and measles has an R0 of that", but it takes all of five minutes to discover that the way it's calculated can't support such statements.
That's why as presently defined it's useless. If you can't compare the values with any other value, what are they for? Put another way, claims about R0 aren't falsifiable.
Epidemiology needs to develop far more robust methods that aren't just applying R-the-software to random datasets scraped from the web if it wants to be taken seriously as a field. There are very basic philosophy of science issues here. Argument by textbook gets us nowhere, because the textbooks are themselves written by people engaged in unscientific practices. The expectation by outsiders is reasonable, the actual way things operate isn't.
Therefore, my suggestion - meant constructively! - is to rebase the field on top of microbiological theory. Scrap the models for now. Delete "and everything else" from the R0 definition and come up with an algorithm to compute a measure of infectiousness from DNA/RNA or lab experiments only. Once you've got a base definition that lets different labs replicate each other's numbers, you can start to incorporate other aspects (under new variable names) like immune system strength, population density grids etc.
Such definitions won't let you give governments predictions of hospital bed demand right away, and indeed may not let you calculate much of real world value for a while, but the field isn't able to do that successfully today anyway. COVID models were all well off reality. What it would do though, is put epidemiology on track to one day deliver accurate results based on a firm theoretical foundation.
The suggestion that SARS-CoV-2 spreads faster than influenza because two studies on different populations at different times found R0 of 2.5 vs. 1.7 respectively is indeed false--that difference is obviously within the expected spread from different environments. I thought the top reply to that comment (quoting Wikipedia) clearly implied that, so I didn't think any further effort there was required. You posted other statements that were false in different ways, so I responded to those.
That said, SARS-CoV-2 really does spread faster than influenza; among other reasons, we know this because influenza cases went almost to zero during the pandemic, implying that the same behavior in the same population that clearly resulted in R0 > 1 for SARS-CoV-2 resulted in R0 < 1 for influenza. That's a relatively trivial and obvious claim, but it's falsifiable and it involves R0.
It's pretty common to reduce a time series to a single number. For example, in economics, it's common to look at a compound growth rate per year, averaged over the period of interest. Likewise, in epidemiology, it's common to look at a compound growth rate per estimated serial interval, averaged over the outbreak and corrected for immunity acquired during the outbreak. That's R0, with all the convenience and all the flaws of any other simple aggregate statistic.
> Therefore, my suggestion - meant constructively! - is to rebase the field on top of microbiological theory. Scrap the models for now. Delete "and everything else" from the R0 definition and come up with an algorithm to compute a measure of infectiousness from DNA/RNA or lab experiments only.
I hope you realize that biologists aren't all stupid? If they could somehow define "infectiousness of the pathogen alone, without environmental factors", then that would be incredibly useful, removing all the factors that complicate comparisons of R0. The fact that they've made no attempt to do so should be a clue that the concept that you're wishing for simply doesn't exist.
They do study growth rates in cell culture, or the amount of virus exhaled by a sick lab animal, or the amount of virus that a healthy lab animal must inhale to get infected with some probability. Those are well-defined and somewhat repeatable lab measurements, but they're not very predictive of spread in actual humans. Computational methods are even less predictive; the idea of calculating infectiousness in humans from a viral genome is mostly science fiction for now. They're trying, but this may be harder than you think.
> we know this because influenza cases went almost to zero during the pandemic, implying that the same behavior in the same population
We don't know this no, what you said here is just an assumption. There's a competing hypothesis (viral interference) which seems to explain the data better.
The way epidemiology currently works just cannot tell us which virus is more infectious. I agree that a rebase onto microbiology would be hard and maybe fail but the current approach has already failed. Doing difficult research that might not pan out is how they justify grant funding in the first place.
> There's a competing hypothesis (viral interference) which seems to explain the data better.
How would that explain why SARS-CoV-2 suppressed influenza, instead of influenza suppressing SARS-CoV-2? If viral interference occurs (which I agree it may), then the two simultaneous pandemics are coupled; but you'd still expect the virus with higher R0 to win.
> > it is recommended not to ... compare values based on different models
> i.e. R0 numbers are worthless. You can't compare these values between pathogens
That conclusion doesn't follow from the predicate. The model isn't a single simulation run. To mathematicians, the model is the entire framework. It's the SIR model, or the SIS model, or the SIER model, or my favorite model of immunity decay against pertussis... _those_ are the models. The virulence of the infection being modeled, resilience of the population, morbidity and mortality rates, rate and timing of population quarantine, vaccine adoption rate, vaccine efficacy, whether any of the aforementioned values are themselves functions of time... those are just parameters into your model. We absolutely compare the values between pathogens _within the same model_ when discussing the utility of the model.
But typically, the utility in reproduction ratio is as a point of comparison as you tune other parameters. This is part of why a comparison of reproduction ratio across models isn't recommended. It's not just that it's hard to draw meaning from the comparison, it's that the base assumptions of the models might be too different for the comparison to hold any meaning. The reproductive ratio between a continuous model with uniform population mixing is fundamentally different from the reproductive ratio approximated from discrete simulation. They may both broadly speak to "if everyone they saw was susceptible, how many people do you expect to get sick per sick person?" But what that ratio means is dictated by the context of the model.
A frequent utility in comparing ratios is to discuss intervention impact. One might write "Our model found that overall reproduction was reduced to a factor of 0.XYZ (comprehensive infectivity parameters a=nnn b=mmm c=ppp) when the population undertook vaccination schedule foo. Conversely, reproduction was reduced to a factor of 0.JKL for the same infection under vaccination schedule bar. See Figure 14 for complete population state levels over time."
That's all that is. It's a number that has some meaning in context, and one that is often removed from that context and unreasonably expected to retain its meaning. Averages don't mean as much if you don't know if your distribution is multimodal. It's the same thing - a summary stat that can give you a glimpse of the whole, but still just a summary stat.
I met the guy (Nick Hengartner) who did the 6 (really 5.7) estimate and knew his colleagues and I can tell you the paper was a lot more careful than that.
Want to explain how they computed it to us? Because if R0 is a real thing then either the people estimating R0=1.something were wrong, or Nick was wrong, and so somewhere some methodologies need to change. I read a fair few modelling papers and R0 (under varying names) was always being used by the model as a free variable used to achieve fit to a historical dataset. It was never being established via lab work, as you might expect given its definition.
So they did exactly what we're saying they do? The paper sets up some ad-hoc models unique to this academic group and then reversed them to find values of R0 that could fit. The problem is underdetermined so there are a huge array of values that could work. Key line:
> Overall, we report R0 values are likely be between 4.7 and 6.6 with a CI between 2.8 to 11.3
That's an extremely wide CI by any measure. It's a bit unclear how this is meant to be a contradiction. It looks like a good example of the issue. There is no universal theory or method for computing R0. Every single epidemiologist has their own unique approach which is then often discarded in time for the next paper, making the numbers incomparable.
There's some minor variation due to different curve-fitting approaches, but the big variation (e.g. R0 from 3.7–203.3 for measles, per my other comment here) is real, simply because the environment or human behavior varied. As others have repeatedly noted, R0 is a function not just of the pathogen, but also of its environment, including the behavior of its human hosts.
Earlier, you wrote:
> It [R0] was never being established via lab work, as you might expect given its definition.
If you expected that "lab work" could establish R0, then you've grossly misunderstood its meaning and definition. It seems like you're looking for a concept of "R0 but for the pathogen alone, independent of environment and human behavior". That just doesn't exist though, any more than you could define the growth rate of a plant independent of weather and soil fertility.
Briefly, as the substance is discussed in my other reply:
> the big variation (e.g. R0 from 3.7–203.3 for measles, per my other comment here) is real
Morpheus: "What is real? How do you define, real?"
CIs that wide are just an obfuscated way of saying "we have no idea what's going on or what will happen". Anyone can make predictions that way. For example by the end my life my bank balance will be $4.7 million (CI $5.00-$50M). Those numbers aren't "real" in any meaningful sense. Anyone can express don't-know in sophisticated looking numerical form, and they wouldn't justify me claiming to be a financial expert on the back of them.
> any more than you could define the growth rate of a plant independent of weather and soil fertility.
You can define growth rate of a plant this way: define a standardized lab environment with regularized soil composition and artificial light/watering schedules. Then plant seeds and measure the dry weight at the end of a fixed time period. This will give you a number that's comparable across species. There are other definitions you could use because "growth rate" is slightly ambiguous in English (does a tree grow faster than a weed because the tree achieves bigger mass?), but that's the general idea.
What you shouldn't do is just grab datasets of wildly varying quality off the internet, fit an equation you just invented on the spot to that data, and announce you've discovered something real about the plants in the data. That would indeed yield a growth rate that doesn't tell you anything meaningful.
> You can define growth rate of a plant this way: define a standardized lab environment [...]
If the standardized lab environment is dry and sunny, then you'll conclude that a cactus grows faster than a fern, since the ferns will mostly shrivel up and die. If the standardized lab environment is moist and shaded, then you'll conclude that the fern grows faster, since cactuses will mostly die for lack of sun. So which is right?
The concept that you're looking for simply doesn't exist--the growth rate of an organism can't be defined except with reference to its environment, which for a virus that infects humans includes human behavior. (What rate of condom use should the standardized lab environment for HIV correspond to? How will you model the increased popularity of fentanyl?)
You are looking for CS-level rigor and simplicity in biology, but biology doesn't work like that. You are correct that many biological results were thus oversold to the public during the pandemic; but you're once again criticizing those public-facing oversimplifications, not any science as a practitioner would understand it.
Neither can be said to be right without reference to a fixed context. If your field standardizes on a lab setup that's drier and sunnier than what ferns like, you'd indeed conclude that ferns grow slower in that context and that's OK because the growth rate is at least well defined. If there's a use case for comparable growth rates in different contexts, OK, define separate names for those rates and measure them separately. Or try to isolate the effect of heat and light such that the growth rate of any plant can be computed from the equivalent of e=mc^2.
Likewise you wouldn't try to measure the infectiousness of HIV in people, clearly. If you want to measure the relative "infectiousness" of viruses in humans using precise numbers then you'd need a controlled experimental environment, presumably something in vitro. That would miss a lot of factors that are important if you're trying to predict epidemics at the society-wide level, but OK, so be it. You need a firm footing of the basics before you can progress to more complex scenarios.
I don't really agree that it's unreasonable to expect CS-level rigor in biology. Microbiologists seem to manage it? It's expected that if two labs sequence the same organism they can in principle get the same DNA sequence, and if they do Xray crystallography on the same protein they'll derive the same structure. So we're not even comparing biology and CS here, we're comparing microbiology with epidemiology. The latter seems to be far closer to a social science in terms of its methods and rigor.
To be clear, it's also fine to do epidemiology using less rigorous methods if it was done in the way it mostly used to be done. When I read papers from the 80s they seemed to be much more appropriate to the actual data quality - largely prose oriented, very limited use of maths, presenting falsifiable hypotheses whilst admitting to the big unknowns. That's fine, science doesn't always have to be precisely quantifiable especially on the margins of what's known. But if scientists do precisely quantify things, then those quantities should be well defined.
> That would miss a lot of factors that are important if you're trying to predict epidemics at the society-wide level, but OK, so be it. You need a firm footing of the basics before you can progress to more complex scenarios.
That's how EE/CS stuff usually works (at least outside ML), building complex systems hierarchically out of well-understood primitives. The life sciences are different. There's almost nothing there we understand well enough to build like that, so almost all results of practical importance (a novel antibiotic, a vaccine, a cultivar of wheat, etc.) are produced by experiment and iteration on the complete system of interest, guided to some extent by our limited theoretical understanding.
This discrepancy has been noted many times; it's just a completely different way of working and thinking. If you haven't, then you might read "Can a biologist fix a radio?".
> Microbiologists seem to manage it?
A grad student in microbiology can grow millions of test organisms in a few days, at the cost of a few dollars, and get all the usual benefits of the central limit theorem. A grad student in epidemiology absolutely can't, since their test organisms are necessarily people. So you're quite correct that it's basically a social science, since it depends on aggregate human behavior in the same way e.g. that economics does, and is therefore just as dismal. Unfortunately it's also the best and only science capable of answering questions of significant practical importance, like whether the hospitals are about to be overrun. I'd tend to agree that stuff like Imperial College's CovidSim has so many parameters and so little ground truth as to have almost no predictive value. R0 seems fine to me though, and usefully well-defined, in the same way that the CAGR of a country's GDP seems fine.
In the life sciences, it's often possible to design an experiment under artificial conditions that will get a repeatable answer, like the growth rate of a plant in a certain controlled environment. It's much more difficult to use the result of such a repeatable experiment for any practical purpose; consider, for example, the steep falloff in drug candidates as they move from in vitro screens (cheap and repeatable, but only weakly predictive) to human trials (predictive by definition, but expensive and noisy). I'm absolutely not a life scientist myself, in part because I think I'd find that maddening; but essentially all results of practical benefit there came from researchers working in that way.
The R Naught is not as complicated as it sounds. If you get infected and pass the virus on to one person, and him to one person, and that person to another person, and this pattern persists throughout society, you have an infection rate of 1. If you pass it on to two people, and on down the line, you have an R Naught of 2. And so on it goes. If it falls below one and finally to 0, the pandemic qualifies as endemic.
The infection rate is always conjectural, not really empirical. It’s impossible to discern without universalized, random, and thoroughly accurate testing, tracing, and tracking. Those conditions have never been met in any country or any pandemic. So what seems to be a measure of an existing reality is really true only in theory, not realistically discernible in the midst of a pandemic. At best, it is an estimate.
Masks are ineffective at lowering the R Naught. Social Distancing might.
I think the lockdown concept as implemented in 2020 was a great illustration of the problem of scale. It's trivially true that if you as an individual avoid all contact with others during a flu season, you won't catch the flu. You can probably extend that to your family, maybe a bit further, but at a certain scale it just becomes impossible (and undesirable) because of individual variations in occupation, lifestyle, risk and infinitely many other factors. And because someone has keep the wheels of society turning. There was no lockdown for supermarket cashiers.
My own government got very excited by the prospect of dictatorial central planning that lockdown mania created an enabling environment for and immediately set about writing all kinds of complicated rules about what food and clothing people were allowed to buy, as well as putting a prohibition on alcohol & cigarettes and imposing a curfew. Pandemic response immediately became a vehicle for imposing by fiat whatever pet policies ministers could vaguely link to it. Years later, they've all been rolled back, but the damage was done, and everyone still caught Covid.[1]
I definitely agree about the schizophrenic restrictions - buying food is fine but God forbid you want to buy socks in the middle of winter (which are sold in the same store)
Similar things happened in Québec. There was a curfew, unless you had to walk the dog. You couldn't buy certain products, but the stores were as much as crowded.
If it was that deadly and every knew someone who died, they wouldn't go outside.
I think the lockdown concept as implemented in 2020 was a great illustration of the problem of scale.
This is not a popular opinion but I think the fundamental mistake of lockdowns, at least in North America, was starting from a top-down approach instead of bottom-up. People are going to act like selfish assholes. We ordered them not to. I think instead of threats, we should have aligned their selfish interests with the public good by making it easy to sue someone for infecting you. Could you prove that in court? 99% of the time absolutely not. But the fear that killing other people might hit them in the pocket book would, in my opinion, have made a lot of the assholes put on a mask or skip that concert.
Agreed, the cost should have been borne by those who did not take sufficient measures to reduce transmission. Similar to how, when you do something dumb in the ocean and need a rescue, you pay the coast guard back if they determine negligence.
It was negligent to live as if there weren’t a huge pandemic.
I was thinking a legal framework analogous to the one used in Texas where regular citizens could obtain ten thousand dollars by suing women who had abortions. Sort of a "turnabout is fair play" approach.
> You can probably extend that to your family, maybe a bit further, but at a certain scale it just becomes impossible (and undesirable) because of individual variations in occupation, lifestyle, risk and infinitely many other factors. And because someone has keep the wheels of society turning. There was no lockdown for supermarket cashiers.
I don't understand what point you tried to make. There were naturally essential workers that were excluded from the lockdown. So what? What's your point?
> My own government got very excited by the prospect of dictatorial (...)
I'm going to cut you right there because you're diving into loony conspiracy territory, and one which was already widely proven to be utter nonsense.
The point of lockdowns is to hinder the spread of a disease so that emergency services had a better chance of coping with the demand without being overwhelmed.
Where I lived, the local government had to commandeer a sporting venue to temporarily store dead bodies. Because hospitals and mortuaries found themselves over capacity.
Some responsible people staid home voluntarily. Others could not stay home because they were front line workers. And then there were the sociopaths and morons who even went out of their way to violate even basic health and safety rules, such as spitting on people on the street.
Lockdowns were sold to the people as something that would stop the spread. If you can get every infected person to infect less than one other person on average, you can stop the spread of an infectious disease completely. At least in theory.
There are two variables here. How infectious the disease is and which percentage of the population can isolate themselves at home without society breaking down.
If everybody stays home you don't have hospitals, you don't have electricity, nobody picks up the garbage, and people will go hungry. Needless to say, that doesn't work. So what percentage of people still need to go to work? And it turns out you need a lot of people to work. From elderly care to daycare, from hospitals to supermarkets and their entire supply chain. And those people will inevitably get sick and infect their family and so the spread continues.
And how infectious is covid? Very, and variants increasingly so.
Which means you can use measures to slow down a disease like covid, but you have no chance of stopping it completely. And that's something some governments refused to accept, and they enacted a ton of erratic and ineffective countermeasures in a desperate attempt to do something impossible, instead of taking a more measured approach focused on slowing down the spread and increasing hospital capacity.
Some people will insist that government policy was in fact reasonable and measured, but it really wasn't. Deutsche Bahn still required masking in January. This year. 2023. I kid you not. It's totally absurd.
> Lockdowns were sold to the people as something that would stop the spread. If you can get every infected person to infect less than one other person on average, you can stop the spread of an infectious disease completely. At least in theory.
No, I do not think so. The curve in "flatten the curve" was referred to the daily number of cases, and the impact it's growth had on saturating health care services. Lockdowns hindered the spread so that services could be able to respond to the daily inflow of new cases.
> If everybody stays home you don't have hospitals, you don't have electricity, nobody picks up the garbage, and people will go hungry.
This is a totally disingenuous and completely wrong strawman, and one that springs either from intentional ignorance or outright bad faith.
No, you don't lock people up and expect everyone to stay in house arrest. You are pretending that the whole concept of "essential workers" didn't existed, let alone was a central point of lockdowns. People were arguing if occupation X or Y should or should not be classified as an essential worker explicitly because that meant either the workers should or should not stay at home.
It was to slow the spread. It was as the parent comment said - to slow the rate of hospitalization so the medical system wouldn't collapse and have needless excess death from lack of capacity.
You're making all valid points and all those points were immediately clear at the start of the lockdowns, for anyone who would listen. Problem is, a lot of people are simply unable to listen to reasonable arguments. That was a problem back then, and they'll remain convinced of their own opinions even in when they are proven to be wrong over and over. It's like people who are religious. You can't reason them out of it.
Herd immunity? Never happened because infection isn't preventing reinfection with a different strain.
If there had been actual, effective lockdowns early enough they might have worked but by March 2020 the cat was out of the bag. Japan's model of universal masking, testing, and outdoor interaction without lockdowns is the best model for the future.
I understood the justification and necessity for lockdowns but not only were they too late but they were also infested with political exemptions and even if they had helped they were only ever a temporary solution.
Full lockdowns certainly wouldn't have been allowed to last long enough for the vaccine to be produced, especially if that research, development and production had taken as long as it was initially expected to take.
The western covid public health response was a bit of a disorganized mess, but even there it ended up being remarkably effective. I was amazed that we had almost two years with virtually zero flu infections, which showed the vast difference between the infectiousness of normal influenza and covid. Unfortunately, covid was such a stubbornly infectious little bugger that it only slowed the progression.
"China did actual lockdowns."
Yes, they did, and literally made prisoners out of their own people. Which had the unfortunate consequence of killing people for lack of care, food and social contact.
"Herd immunity? Never happened because infection isn't preventing reinfection with a different strain."
This is exactly wrong. Once you get covid you may contract a different strain, and if you are a normal healthy individual it will be like a bad cold, if you have symptoms.
Exactly re China: my point is people should stop describing the US response as lockdowns because they literally never happened.
Re reinfection, good luck with that. Every time you catch covid you have a one in ten chance of long covid, and that's the current conservative estimate in meta analyses.
In order to calculate a one in ten chance of anything would require you to know two numbers. In this case, you would need to know the number of people that have contracted Covid and the number of people that have experienced long covid symptoms. I can guarantee there is no possible way to know either number so anything is probably a grossly inadequate estimate depending on bias.
I love watching people argue over COVID-related politics. It's such a perfect example of how tribal politics and scientific illiteracy affect public opinion and unfortunately, all too often, public policy.
I went out of my way to study especially some of the mathematics used for modelling projections into the future.
I not only read about the SIR model, but poked around a few of its variants like SIRV, SEIS, MSEIRS, etc... I even ran a few up in Mathematica and toyed around with different parameters, trying to get a feel for how the errors accumulate and what can and can't be predicted.
Just that little tiny corner of the pandemic response is insanely complicated once you get into the weeds. You have to account for what fraction of the infected actually turn up for test. What fraction of the tests are false positives or negatives. How fast mutations spread and distort the test results. How other countries or even counties report their statistics differently. And so on, and so forth.
Once you get a good feel for a tiny part of the big picture like that, it makes it much easier to gauge who's spouting bullshit, and who's also been in the same weeds as you have and is covered in cuts and leeches.
At the end of the day, the numbers said 'x'. Everyone that sounded like they knew what they were talking about agreed with 'x'. Everyone who sounded like they were making things up to suit their selfish agenda never used terms like MSEIRS, "infection-to-test ratios", or any such thing. They also seemed to use many different numbers, sometimes making up new numbers in the same conversation. More commonly, they wouldn't use numbers at all, and talked instead about freedom or human rights. Emotions and feeling that might get hurt.
Here's a number: so far at least 6 million people have died, of which 1.1 million were in the United States alone.
The numbers said it would have been a lot worse if prompt action wasn't taken. Ten times more deaths or even worse were entirely within reasonable projection bounds.
Yet... people keep arguing as-if 6 million people hadn't died. As if hospitals hadn't been overwhelmed. As if we lived in some sort of counter-factual universe, or we could choose to live in such a place through sheer force of will.
As if we could berate the virus into not mindlessly replicating exponentially in order to appease our God-given right to freedom and profit.
I love it when people that didn't look at how accurate the numbers behind the death toll speak to how big they were. The numbers are crap and they can never be anything other than crap by design.
Did you know that not one healthy individual under 30 died from Covid?
Yet, we locked them down, took away their education and ruined their social development at a young age. Shame on you.
This article immediately claims that the Asian Flu in question was far deadlier than COVID. This is categorically false.
In fact, it's not even close. The article claims 116k US deaths attributable to the Asian flu. Meanwhile, there were 10x that number of excess US deaths during the COVID pandemic.
As others have pointed out, the AIER is a conservative think-tank. I don't know where they're getting their casualty numbers from, but it's not from any reputable source.
This is clearly biased garbage.
Edit: COVID directly caused 1.1 million verified deaths in the USA. We were second in the world in COVID deaths as a percentage of the population.
You are comparing those numbers directly, but that's not how you compare those numbers.
First the population size, as per the article, was half what it is now. So you can either double the asian flu deaths or half the covid deaths to account for this.
That still leaves a huge gap, but this is where demographic analysis comes in.
Usually you see this as age adjusted deaths.
In this case, the population of the US has been aging for a long time so you would expect more deaths from covid than the Asian flu for an equally deadly virus.
The other demographic change that is important, especially when talking about covid is rates of obesity, which is something else that has grown over time in the US population.
That's a really long winded way to say you can't just compare raw numbers.
The article doesn't give an explanation of how they came to their conclusion, but if you take population size, age distribution, and obesity rates into account, I could see the adjusted numbers being close.
Yes, there are more obese and elderly people now than there were in 1957. No, we can't "adjust" death numbers to place less weight on the deaths of those obese and elderly people in this context. Perhaps it would make some sense to do so if our goal was to measure virulence of the virus, but policy decisions have to take into account the composition of the population as it is today.
>if you take population size, age distribution, and obesity rates into account, I could see the adjusted numbers being close.
Those are confounding factors, but I think it's quite a stretch to believe they would provide a 5x adjustment (after accounting for 2x population), especially if you also adjust for the drastically improved quality of and access to healthcare, which would skew the adjustment in the other direction.
Obesity rate is 4X what it was back then. So 2X for population, 4X for obesity, and then however you want to calculate the additional increase for an aging population. 10X ain't that crazy.
I would agree, but we're talking about 35 to 40% prevalence of obesity and all the attendant diseases caused by it in the US. If the next wave of the flu or pneumonia would kill those same people who were pushed over the edge by COVID, would you be for lock downs and business closings in these cases too? Because that's what happens whenever a person with that many comorbidities gets an infection like the flu or pneumonia and they are over 80, just like COVID. Diagnoses of obesity changed during this period too due to fat-shaming blow back. A lot of excuses are made for these actions saying any criticism is in hindsight, but there were scientists being censored and suppressed who were raising very good points with early data and reference to past social measures during pandemics too. The memory-holing of natural immunity in those who already had COVID, was almost criminal by the CDC and others. SARS-CoV-1 immunity studies were being conducted on survivors of it from 2003 for over 18 years and they still showed antibodies or immunity traits from natural infection. Even though, SARS-CoV-2 is pretty much believed to have been enhanced in the WIV at this point with an accidental lab leak causing it to spread worldwide, why wouldn't it have similar correlations with it's sibling virus re: natural immunity? Having contracted COVID in my mid-fifties and it being no more than the flu for me, I decided not to get vaccinated when it was becoming scary that I may lose my job for this stance and being stigmatized by all of my fellow workers. I did not argue against the vaccination in the vulnerable and those who didn't ever have COVID, but I had it, and I went with the overwhelming precedent of natural immunity as something that had always been recognized by the CDC and others (funny how the definition of natural immunity was edited over time on the CDC website to fit the narrative and push for vaccination). Glad I stuck to my guns and not to the mob's. One of the loudest voices at work rushed for all of his boosters and had COVID twice and was ill enough to take off work for a week for each incident not just because of quarantine rules, since he was working from home. Sadly, my nephew in his early twenties at the time received the vax and was rushed to the emergency room by ambulance with myocarditis, and to this day has follow-up appointments to track his cardiac health. He is a runner, athlete, with no previous medical conditions. Statistically, he was not even in any significant risk category.
>Sadly, my nephew in his early twenties at the time received the vax and was rushed to the emergency room by ambulance with myocarditis, and to this day has follow-up appointments to track his cardiac health.
>Among 192 405 448 persons receiving a total of 354 100 845 mRNA-based COVID-19 vaccines during the study period, there were 1991 reports of myocarditis to VAERS and 1626 of these reports met the case definition of myocarditis.
Myocarditis is one of very few side effects from the vaccine, all of which are vanishingly rare. It's well understood that the vaccine was highly effective in reducing the severity and spread of COVID and is one of the safest vaccines ever produced.
>How well it works: Moderna’s initial Phase 3 clinical data in December 2020 was similar to Pfizer-BioNTech’s—at that point, both vaccines showed about 95% efficacy for prevention of COVID-19. Later data on real-world effectiveness for adults showed that the protection from the mRNA two-dose primary series wanes over time, but booster doses bring the immune system back to robust levels.
You didn't ignore the mob, you ignored the science. You listened to a mob of your choosing, and now you are misinformed and continuing to spread misinformation.
My main point was how they pushed the vax on people even when existing data showed young, healthy (which means no obese, diabetic, hypertense individuals), males were not at sufficient risk to mandate it in universities and push it on everyone regardless of the obvious data by age group, health, and susceptibility. That is not science. That is social policy and politics in the face of common sense. Please stop co-opting the word "science" in this manner.
I have had all of my children vaccinated with the standard course of immunizations, but I am glad I held off on this new vaccine. My children had COVID, and they are healthy by definition. Tell me how acting on common sense, the history of natural immunity in science, and data that was readily available on who was susceptible to COVID very early on contrary to what "The Science" (aka Social Policy and Politics) was saying , is listening to a mob? Use the same date source you used to pull your VAERS numbers and see how obvious it was who was susceptible by a margin early on, and maybe you'll be able to understand how I arrived at my decision to not vaccinate my family who already had COVID.
>...and is one of the safest vaccines ever produced.
This December 14, 2023 will be three years from the first vaccine given. "one of the safest" is a blanket statement and "one" although a quantity is non-quantifiable in that sentence. The article you site is from data collected from December 2020 to August 2021 only 8 months from first vaccine. Pfizer vaccinated their control group from the initial vaccines, so that long-term study was squashed by Pfizer. And the adverse effects data are still being collected and examined in light of reporting criteria and classification. Yet, the blanket policy to vax everyone without prioritizing by harm-benefit analysis and ignoring the science was not just negligent but intentional to push a social policy over the data. Three years is not long-term in the vaccine world. Tell me, if a long-term effect comes up like higher incidences of leukemia or other diseases or undesirable side effects 5 to 7 years from now, will you look back and feel good about the non-scientific pushing of a vaccine on those who were well outside of any reasonable benefit-to-risk ratio? I am glad my young children didn't get the vax. None in my family have had another COVID symptomatic infection or tested positive since we had it the one time. Meanwhile, "healthy" coworkers with 2 or more boosters have had multiple infections with loss of work even when working from home because they were that sick. So do you agree with vaccines and boosters for the non-susceptible demographic who have already had COVID? I'd be curious on your viewpoint on this.
UPDATE: Paper showing a 1 in 35 (22 out of 777, or 2.8%) myocardial injury of 777 eligible participants of an original 1871 employees of a hospital after receiving an mRNA-1273 booster [1].
This is only after 3 years of the vaccine's first dose. That is a pretty large percentage - 2.8%.
I sadly expect to see more and more of these studies with other unsettling results. To the universities who pushed it upon the healthiest of us, they should be ashamed of saying they did it in the name of science when young people were the least affected, and the elderly could be prioritized.
I think this depends on the disease. Some diseases impact the young more than the old. The calculus required to compare age adjusted deaths by the demographic curve of mortality by pathogen is probably complex.
But I would also note that when you are dying or your loved ones die waving age or obesity adjustments to claim it’s not that bad doesn’t work very well. 1.1m deaths is still 10x more, and even on a per capita, it’s still 5x greater net “mourning.”
Whether the same pathogen would have been worse in one decade vs another I think is sort of irrelevant. The public health goal is the reduce mortality over all.
(N.b., I recognize you probably didn’t mean to minimize anyone’s loss - but I am trying to make the point that demographic analysis might or might not be explanatory of the severity of 2020, it doesn’t make 2020 any less severe)
> We were second in the world in COVID deaths as a percentage of the population.
I am not trying to change your argument in anyway but that specific statement is not correct or its using different numbers than direct COVID deaths. The US is 15th. Peru was #1, and EU members Hungary (#3), Croatia (#6), Slovakia (#10), Greece (#13) and Romania (#14) are all ahead of us.
Thank you for the correction! I see now that the full dataset is available in the table at the bottom of the page. I was referring to the chart at the top of the page, which (for some reason) leaves out the 14 countries between Peru and the USA. I wish they wouldn't do that.
So Ebola virus is not as deadly as COVID because fewer people have died from it? "Deadlier" can mean a whole host of things: infection fatality rate of a disease can be far higher even if the total deatg toll is lower, if fewer people contract the disease.
Which is deadlier, being shot in the head with a .50 cal, or catching the flu?
The former is much deadlier - it's basically guaranteed death - but the latter is so much more frequent that it claims more lives even though the vast majority of people survive it. Usually "deadlier" refers to the chances a given event will kill you if it happens, not normalized for the frequency of those events.
The flu most certainly claims more lives, but I doubt most people would agree with the sentence, "being shot in the head is less deadly than the flu."
Sorry I think you’re confusing “deadlier” with “more death,” deadliness is a measure of likelihood of dying when exposed to the situation. Something can be much less deadly yet more people are exposed to the situation and it causes more death. Ebola is undoubtedly more deadly than covid. But it’s much less virulent, partially because it is so deadly. There’s no super spreading symptom free stuff going on with Ebola. Just death.
Yes, MERS killed less people but had R0 estimates from 2 to 5 based on the Saudi and South Korea infections. MERS killed 936 people with a CFR of 36%. The US has an observed-CFR of 1.1% due to COVID-19 (close to Canada with more stringent measures), and Peru, the highest, at 4.9%.
In more visceral terms, if the doctor says you either have MERS or SARS-CoV-2. What is your first thought, question? Which is more deadlier?
Well if they lie so readily and deeply, debunk their arguments themselves. It shouldn't be difficult. It's tiresome to see constant dismissals of points of views based on an obsession with bias. Bias is inherent to most organizations and people, so weight of argument and its evidence is what should count. Going on about the GOP doesn't help either, it shuts down debate dishonestly and ignores the simple fact that many sources from the left of the spectrum are no less capable of dishonest arguments, lies and forcing through their views, complexities be damned.
edit: Also, there's nothing inherently evil or nasty about this organization having the views it does. Their being divergent from progressive liberal views, such as those espoused by many organizations with a left bias, doesn't make them shitty per se.
I agree with a lot of what you’re saying but their bias isn’t just their ideology, the article itself is just false with bad math. They claim at the beginning the avian flu was more severe and wave hands at population growth to explain how 1.13m deaths in a 331m population is less severe than 0.116 deaths in a 159m population. No where do they quote the covid death toll, nor the actual populations at the time. This is presumably because they intend to mislead their readers with an overt falsehood. That is lying, and lends credence to such a stark bias they’re willing to directly lie to deceive their readers into believing their points. These were essentially the only actual facts quoted in the entire article.
Over the span of 3 years. To put this in perspective a typical flu year claims ~40K people each year. So Covid over this time span killed about 10X as many people as a typical flu year.
If you told people "hey, this year the flu is going to be very bad, probably killing 10 times as many people" would the average response be to close schools and many businesses for over a year? Or would the response be to limit lockdowns to vulnerable populations, rather than blanket lockdowns on most of society?
If hospitals said "we're about to run out of room and stop treating everyone" then I would go with whatever prevents that scenario.
edit: COVID placed a 20x burden on hospitals versus the flu even with lockdowns. That's without counting the increased difficulty of treating a novel disease, and increased time in hospitals for covid vs flu.
The notion that hospital capacity had a significant effect on the fatality rate is not so strong. Even early into the pandemic, hospitals stopped putting people on ventilators since it didn't improve health outcomes. So "flattening the curve" just meant extending lockdowns and probably not saving any lives.
So what you are saying is that it was known how many people will be killed by covid-19 before any measures have been put in to affect and that those measures had no influence on the number of those who died? If not, what is the point of your post?
Before March, sure no we did not. But by mid-late 2020, yes we did. But lockdowns continued well into 2021. We had studies to determine the infection fatality rates in mid-late 2020: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7947934/
Ionnadis was slammed for claiming such a low IFR of 0.27%. But later studies have since reaffirmed his estimates: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9613797/ Even when restricting the analysis to the period before vaccinations, the IFR was between 0.3% and 0.4%. Ionnadis was way closer to the mark than the claims of 1.0 or 1.5% IFR that were common at the time.
This mindset is a comfortable position for people to retreat to when they don't want to discuss a situation rationally based on information known at the time but rather want to retroactively push a personal agenda.
Regardless of everything else, I don't think lockdowns could have ever been an option in a pre-internet society or even a pre-smartphone, pre-social-media society. So, say, before 2007 or so.
The day after waterloo europe was filled to the brim with brilliant generals, who with perfect information knew how the batlle could have been turned around and the day won.
My bet here is that lockdowns, while originally intended to "flatten the curve" (and that was a good idea), turned out unexpectedly effective and appeared to reduce infection rates so quickly, especially in the beginning when people were very afraid and lockdown rules were strictly adhered to, that someone got an idea of just resolving the problem altogether by doing "lockdown to elimination", until it became evident that you can't lock down every country in the world unless you threaten/use nukes, and shutting down travel indefinitely is also not possible, and the whole thing became a charade.
Lesson learned for the liberals is to listen to those on the right at least from time to time. If they sometimes behave like idiots it doesn't mean they really are. Republicans got it right on the Covid question.
I think when you talk about Sweden, you've got to remember that they do have things like legally enforced sick pay (if you're ill, you stay at home and your employer has to pay you some proportion of your salary) and high quality government funded healthcare. They have a low-ish population density and social norms that give people a _lot_ of personal space when in public. So the experience that Sweden had with no lockdown is not necessarily the same experience that the USA would have had, where most people dont get paid if they are sick and dont go to work.
Sweden has a low population density because it's geographically large (by European standards) and has only 10.2 million people. However, maybe you forget that it's population is also 88.49 percent urbanized, so they are actually quite crowded together, in a way comparable to many American levels.. It's not like those millions lived scattered all over the landscape.
Compared to Norway and Denmark yes. And of course there was a lockdown in Sweden. Just less strict than in most other places. But it was not business as usual in Sweden. I assume you will now tell me I'm wrong about that despite I'm being in Sweden and you probably never even visited?
I'm wondering how a reading of that article could lead anyone to quote it as an example of 'no lockdowns' - its very explicit that in many ways the measures taken in Sweden were even more restrictive (after 2020) than its neighbors in Norway and Denmark - both of which fared better than Sweden, both in deaths-per-million and also in the effect that the pandemic had on the economy.
The truth is that while the initial (and quite brief) open policies were in place, the authorities mistakenly thought that herd-immunity was close to being achieved, and that the astronomically high number of deaths (at several stages, the highest number of deaths-per-million in the world), were worth the reward of achieving it. The government even had one workshop where they discussed with relevant authorities how they would handle the negative press from other countries when Sweden could announce they were 'over' the pandemic (this was naturally before the catastrophic fall and winter of 2020).
After the deadly winter, the government more firmly took the reins from the health authority, and people outside Sweden would be surprised to hear how many restrictions were actually in place: including bans on group meetings, caps on the number of people who could enter a store at the same time, high school kids studying from home, and so on.
But most of all, Sweden is a country where people have lived with 'social distancing' for centuries: Stockholm has the highest number of single-person households of any capital city in the world, and that pattern is repeated all over this sparsely-poulated country. In the summers, a vast number of people leave towns and use their summer-places in the countryside - another tradition that's been going-on for the last couple of centuries. In the summer of 2020 I was in Stockholm, and would often be the only person eating in a restaurant that would normally be packed with people.
All of these factors helped Sweden to keep down what would otherwise have been even more catastrophic numbers of dead. Which isn't to say that the number of people who did die - often without any medical care whatsoever in the case of many elderly people in homes that were supposed to be somehow 'protected' from the pandemic - is not a massive tragedy, that Swedes themselves hardly talk about any longer. Because it really was both a callous loss of life, and a traumatic triumph of selfishness over common welfare.
> The American Institute for Economic Research educates people on the value of personal freedom, free enterprise, property rights, limited government, and sound money
It's not necessarily that they're bad it's just that they're likely not a valuable source of acquiring information outside of what supports a specific position. Like I wouldn't necessarily trust an oil baron to tell me about how global warming doesn't really exist, or I don't necessarily believe Disney's Iger to tell me about how the writing and acting strikes are entitled whining nonsense.
...and the only legitimate source to ask about climate change is the Sierra Club.
and the only legitimate source to ask about the need for copyrights is Disney.
It always cuts both ways. Just because they're against the position you think is obviously correct doesn't mean that you can dismiss a dissenting position. Every story has another side to it. (Well, except this one :) )
I mean, it applies to everyone. The more interesting question in this context is, which of the two groups does it apply to more?
If I have to put both the average CEO and the average epidemiologist on a spectrum of "more interested in my well-being" to "more interested in my pocketbook", I know where I'd put each one.
For a barber, more haircuts = more money. Trying to imagine what kind of relationship you think epidemiologists have with money? It's not like they get a nickel for every person they save from getting sick.
Not everything is purely about money. People are highly motivated by a sense of power or prominence, by a sense of belonging in the "correct group", and by a sense of being useful or productive at their profession. A barber as much as money will believe their haircut will make you look good.
As a thought exercise, I wonder to which group an epidemiologist would need to belong to have a sense of power? The group that says that there is a dangerous disease or the group that says that it's not particularly dangerous?
PS: For people who wonder, the H factor-style ranking mechanisms for researchers means that your rank is higher (which tends to translate to more interesting work and/or more money) if you're heavily quoted by other researchers.
Of course, the easiest way to be heavily quoted, unless you're already a highly established scientist, is by being contrarian/provocative, so that other people feel like they need to debunk your writings.
I'd think in this case it's about the response. What group of epidemiologists wouldn't get a sense of power, prestige than having daily Whitehouse meetings, continual press coverage, and effectively setting public policy based solely on their subject of expertise? That essentially hits on all three points I gave.
The issue is that they'll fail to appropriately consider the broader long-term effects of lockdowns. Most of the advice and policy also wasn't scientifically based in that the effectiveness wasn't well researched, so H-factor scores wouldn't play much of a role.
> I'd think in this case it's about the response. What group of epidemiologists wouldn't get a sense of power, prestige than having daily Whitehouse meetings, continual press coverage, and effectively setting public policy based solely on their subject of expertise? That essentially hits on all three points I gave.
That is definitely one possibility. The other possibility being that a group of contrarian epidemiologists would get power and prestige by claiming that the first group is biased. This has happened in France, with Raoult growing a cult-like following.
> Most of the advice and policy also wasn't scientifically based in that the effectiveness wasn't well researched, so H-factor scores wouldn't play much of a role.
Well, in that case, H-factor-style scores wouldn't play much of a role because this was not research but policy.
I seem to remember that the effectiveness of lockdowns on diseases has been pretty much proved way before covid. Of course, their effect on economy may not have been studied quite as well :)
No, but understanding the position of the author is useful. There is an agenda behind this article. If my goal is to avoid death during a pandemic, personally I would rather read articles about pandemic response by epidemiologists rather than economists.
Towards an individual those things may be fine, but we each live in a society, and how your actions effect others could be a factor in how much each of them may be exercised.
Certainly not! The fundamental problem is that arguments written from a naive perspective of assuming/asserting we have these things, while we most definitely do not, end up advocating for horribly oppressive policies.
The current government policy is that most everyone should be continually working around 40 hours a week, enforced by a financial treadmill created by continual monetary stimulus. So this noble idea that people could have individually chosen to self isolate or freely associate is fallacious with our current setup. Without "lockdowns" (aka closing businesses), most people would have been forced to keep going into work for business as usual, just as they do for other communicable diseases until the symptoms cannot be ignored.
Centralized control begets more centralized control to address its own failings. Focusing on surface issues while ignoring their underlying causes just makes you end up being a tool for entrenched interests wanting authoritarian policies that benefit them.
Personal freedom can be a bad idea in crisis situations. Selflessness and following procedure can be better for the collective. This is why crisis operators follow checklists rather than giving each individual absolute personal freedom.
and there's the temptation to govern in a permanent crisis mode. there is no end to reasons why there is a crisis. or, is there a scientific definition of "crisis"?
Yes, I agree that there is a temptation for those in power. Legal frameworks can be created to try and limit the lengths and conditions under which a "crisis mode" can be enacted, but there will always be people looking for more power.
If anything COVID demonstrated the opposite - governments were all too eager to get back to BAU despite the situation still being severe, resulting in notably high excess death rates.
Politicians are experts at that surely. But in this case I'm not aware of a case where any epidemiology or other public health policy experts were telling governments lockdowns needed to be ended.
The cynical side of me suggests that there were too many at high levels of government who felt that lockdowns impinged on their ability to enjoy the levels of power they were accustomed to, and so the opinions of those whose job it was to advise on such matters simply got overridden.
Absolutely false. If the government is going to abridge my rights, such as forcing lockdowns or vaccinations, they better show me the necessity and efficacy of those abridgements. The government can't just come in and say, "This is a crisis, we get to do whatever we want." Fuck that. That's how authoritarians are born. Many closet authoritarians took advantage of covid to become dictators without any evidence of efficacy of their mandates.
If I started shilling for the Marxist-Leninist Institute of Vkou that promoted cake for everyone, equality, unity and prosperity, self-determination and social wellbeing, would you be concerned about any of those things separately, together, or would you just dismiss me out of hand, because you think you know where that road leads?
I think I know where the road of 'personal freedom, free enterprise, property rights, limited government, and sound money' leads, and I'm also usually quite happy to dismiss anyone shilling for it out of hand.
Marxist-Leninists often have fair and valid critique of society. Hearing them out is valuable even if you (like myself) find yourself opposed to many of their values and proposals.
Not in an absolute sense: property rights are obviously very important to how society functions. But "the US needs stronger property rights" is in general a harmful position. US limitations on property rights are largely to tax the ultra-rich and to limit exploitation and concentration of wealth. For example, tenants' rights are pretty much directly opposed to the landlord's property rights, and tenants' rights do not (IMHO) need weakening in most places in the US, but instead need strengthening.
The same holds to some extent for the other values, but maybe only in context. (Personal freedom to do what? Not to get an abortion...)
Also, we're talking about a website with a front-page article arguing that reparations for slavery + Jim Crow + other racist discrimination are bad, because slavery is "like winning the lottery" for modern American black people. After all, without the system that kidnapped and enslaved their ancestors and then discriminated against their grandparents and parents and still discriminates against them today -- such that they have less income, less savings, worse life expectancy, triple maternal mortality etc -- they probably would have been born in Africa!
... but if they were, it wouldn't be the first time. These guys are also global warming denialists, covid deniers, and they even vociferously defend third world sweatshops.
It's also an organization widely derided as disseminating misinformation about climate change and COVID-19, its two major hobbyhorses. This is a strongly biased source of research dissemination.
Oh wow this is such an idiotic article I do not know what to say. One of the excuses they used is that hey the virus is already here and spreading so why the lockdowns?
For context, the US had just gone through a polio epidemic, starting ~1949.
Before Salk's vaccine was discovered and widely used (~'54) there was polio hysteria, public places were avoided, "unclean" Italians were shunned, as were cats. It was a ridiculous overreaction. Too soon for anyone to be fooled again.
Strangely, none of that is mentioned in an article about US reaction to a pandemic just three years later.
This article seems to be hoping people will ignore differences between the two pandemics even though we just lived through one of them:
* Covid killed far more people. One estimate for global deaths for the 1957 flu is 1.1 million—around the number of deaths from COVID-19 in the U.S. alone
* COVID-19 hospitalized more people. Apparently, the 1957 flu did not overburden hospitals. Even with efforts to “flatten the curve,” COVID-19 did.
* COVID-19 is a longer illness. While some people recover in 3-5 days (the article’s estimate for the 1957 flu), 5 days is the minimum isolation period and longer recoveries (not even factoring in Long COVID) are common.
* The vaccine was available earlier in the pandemic’s course, at least in the U.S. According to a Smithsonian article [0], a vaccine researcher was able to convince companies to start manufacturing a vaccine before it became widespread in the U.S.
It also ignores the fact that despite not locking down in 1957, the U.S. went into a recession anyway.
The WHO has global deaths at up to 30 million, most of which are in the staggering incrase of excess deaths the past 1.5 years. Then we have over 100 million with Long Covid officially and it's growing at a staggering rate too. In a lot of countries 1 in 5 have new Covid related health conditions.
It's a bit early to be calling it over given its hospitalising millions world wide every week, killings 100s of thousands and disabling millions still. It's a lot worsen than Flu by the numbers so far and it's still successfully raging.
1 in 5 is probably an overestimate, but even the lowest estimates of Long COVID prevalence are alarmingly high. Honestly, even if there wasn't a single new Long COVID case starting today, the fact that many still haven't recovered would make it a significant ongoing health issue.
I agree it's not over, but saying it's raging is not correct either. In the U.S. excess deaths are close to zero [0] and hospitalizations are also low [1]. Other countries largely seem to be seeing similar patterns, although I have not looked at their numbers as closely. We could see another wave, of course, but currently we are in a lull. For what it's worth, I think there are still precautions that make sense because they are are effective and relatively low-cost, like masking in crowded indoor spaces and testing before and after attending large events.
Linked article claims that a vaccine was developed late and had minimal impact.
Elsewhere, the case has been made that the vaccine was developed and deployed rapidly before the virus took full hold, and halted the pandemic in its tracks.
AIER seems to be a Conservative/Libertarian think tank that's anti-climate science, among other stances, including anti-lockdown (what this article is about).
He's implying that we should be more skeptical of articles from sources that have gotten basic science wrong in other articles.
It's not a liberal vs conservative thing per se. There are plenty of liberals and progressives who get basic science wrong. Liberals are more likely to reject nuclear power or GMO food for reasons that are not scientifically justifiable, for example [1]. Liberals have historically also been more likely to believe in medical nonsense like healing crystals and homeopathy and anti-vaccination.
The things liberals are more anti-science on though are also less likely to be the kind of things that require national or international solutions and so attract fewer think tanks.
Hence there is a better correlation between libertarian/conservative think tanks and scientifically unsound positions than there is between liberal/progressive think tanks and such positions.
[1] There is a decent argument against GMO food in places where food is abundant and cheap so avoiding GMO doesn't mean famine, but it has nothing to do with the science of GMO itself. It is that GMO gives food companies much more ability to customize and tweak foods in ways that are great for business but bad for public health. We already know when it comes to money vs health they go for money, which is a big contributor to rising obesity. They can still accomplish many of the same things without GMO that they would use GMO for but it is slower and more expensive which reduces the amount of harm they can do and gives more time to get regulations to catch up.
This is from a conservative - right wing propaganda outlet.
That being said, what happened in 1957-58 doesn't really apply here. First, population density wasn't nearly what it was today. It was the land of single-family homes and automobiles, not high-rises, dense air travel and public transit.
Secondly, the lockdowns were necessary to prevent the healthcare system from collapsing. Rate-limiting the illness with lockdowns and other NPIs allowed hospitals to remain functional and adapt to the crisis. In Italy at the onset of the pandemic, the Italian healthcare system dealt with collapse and rationing of care, with physicians choosing which people to treat and who to leave to die.
Besides the economic harm and potential developmental harm induced by closing schools for kids, I think lockdowns did incalculable social harm to society. It gave huge swaths of the population a grudge against the system, a chip on their shoulder that won't go away anytime soon. It burned up goodwill and trust for experts and politicians (who generally didn't have much to spare in the first place.) And coupling this with social isolation at the same time made a lot of people become frayed around the edges if not outright insane.
> I think lockdowns did incalculable social harm to society.
I don't know about society, but this was the straw the broke the camels back for me. I have not been the same since, I don't think I ever will be. The first lockdown in my province was when things really started to go wrong for me mental health wise in a major way and it only got worse as they continued.
What's really been maddening is that people get angry when I mention the affects it all had on me, they assume I'm taking a political stance first and foremost, they tell me it wasn't that bad, and they try to tell me I didn't experience what I experienced or do what I did.
I used to think things could get better, but I really don't see a happy ending for myself anymore.
You're not alone. Today, every decision that I make is done with the objective of insulating myself non-violently from future coercive actions by the state similar to those during the coronacrisis. For example: expenses, domicile, career, voting.
I know many similar people, formerly of all different political, philosophical and religious persuasions. My rough estimation is that this voting bloc is between 20 and 35% of western society.
To those who disagree: although we are products of the same society, we have simply a fundamentally different view of liberty, happiness and risk tolerance.
And yet some of us actually liked that period of time where we were at home more, had more time to do things like bake bread, cook actual meals, read, etc. I think in my case my mental health declined for different reasons: As someone with health anxiety in the best of times, it started to dial up to 11. This was not even related to "lockdowns" - I had no desire to go anywhere where people congregated. The fact that there was a contagion out there and that there wasn't really any way out of it (until the vaccines showed up) was what led to many people's mental health decline.
There already was a chip on the shoulder of a large number of American and that has been fed and grown by certain media and social channels specifically to undermine trust in institutions and checks on power. The lockdown (that wasn't locked down) was just more fuel on that well-feed fire.
> fed and grown by certain media and social channels specifically to
Ideologues are always saying that anybody who doesn't agree with them must be brainwashed. They can't imagine that could actually choose to hold a different point of view from their own. Well let me tell you it ain't necessarily the case.
Always blows my mind when people suggest the only reason someone wouldn't trust the US government is because they've fallen for some misinformation. The US government does a great job of destroying trust all by itself.
It's really odd seeing comments on HN upvoted like:
US government overthrew Iran democratic government -> "I know the US is so evil!"
US government secretly injecting US citizens with radioactive material -> "My gosh, what's wrong with these people?"
US government lies about reasons for Iraq War -> "One of the great crimes of the century"
Then someone suggests, that just maybe, the lockdowns weren't based on science and that we should be concerned about the government overstepping and the comments are suddenly -> "Wow, did you forget your tinfoil hat?" or "Why don't you believe in science?" or "Think of the children"
It's really weird. The US gets rightfully condemned for wrongdoings, but then suddenly any suggestion that they did it again is met with violent opposition.
They are propagandised to the gills. Their brains will break and they probably won't be able to function anymore if they try to go through all the contradictions.
Exactly. Initially "lockdowns" (and I hesitate to even call them that here in the US, we didn't have literal lockdowns like China had where they welded doors shut on apartments) were seen as positive - "flatten the curve to help our healthcare workers and keep our hospitals from being overrun". Pretty soon, though, they started getting very negative framing from right-wing social media, etc.
>and I hesitate to even call them that here in the US, we didn't have literal lockdowns like China had where they welded doors shut on apartments
Were there even places that gave you a citation for being out "uneccessarily"? Every single "lockdown" I'm familiar with in the US was voluntary. There was a period where "non-essential" businesses were forced or encouraged to not operate, but even that still isn't a lockdown, and nobody was forced to stay in their home.
Yes, the word lockdown means forced quarantine of the entire population by law (except "essential" workers). Were they really voluntary everywhere in the USA? For example, the UK is still processing a giant backlog of fines and imprisonments for people who violated lockdown rules, more than 28,000 so far. You were allowed to go for a walk alone or with members of your household once per day, and go to supermarkets, but nothing else.
afaik, and certainly nowhere around where I live (Montana), there were no UK-style lockdowns in the US. Here we had: schools closed, theaters closed, and restaurants closed for indoors dining, and we had quarantine rules for people moving from out of state (that were not enforced). No restrictions on leaving your home, shopping, etc. No enforcement/fines.
In the lefty commie California Bay Area where everyone "believes in the science", I was never, ever stopped by the lockdown police to ask why I was outside. I don't know why the UK issuing thousands of fines is relevant to this discussion.
Fair enough, then it's not relevant and I shouldn't have brought it up. I think a lot of people in the rest of the world don't realize how much less totalitarian the restrictions were in the US.
In the thick of it I felt like the lock-downs were probably necessary in the beginning of "flattening the curve".
Many around my parts were being outright belligerent asshats when all we had was asking nicely that people distance and wear masks. A substantial subset of the population did the exact opposite, and caused all sorts of trouble being antagonistic even to people just trying to buy groceries.
Then the lockdowns happened and it was like a light switch. I rarely saw the same kind of troublemakers acting out that way in public. Apparently once the US starts gutting its own economy to deal with an invisible threat, people start taking it more seriously. Until then it was like they thought it was all fake news, running around mocking the gullible masked suckers.
But why they didn't end far sooner, like maybe once food supply chains were recovering and our shelves weren't empty anymore, is totally beyond my comprehension. It evolved from "flattening the curve" to "prevent as many deaths as possible at all costs", which IMNSHO is where it went all wrong.
My personal chip developed when—almost overnight—gathering in large groups went from something reckless akin to drunk driving to an essential activity.
Do what you want, everything has tradeoff and risks. But don’t pretend science is normative until it becomes inconvenient.
Businesses were closed, schools were closed. I had to stop my weekly routine of spending Saturdays in the public library because the doors were locked and books were only being lended through the website. The only way to meet and socialize with people was online. Even city parks were "capacity limited", they put police tape around the duck pond because ducks became an attractive nuisance. I had to queue up around the block to buy bread like it was the damn Soviet Union because the grocery store was only letting 10 people inside at a time.
Call it what you like. You're arguing semantics when you say it wasn't a lock-down, but whatever you call it, it harmed people socially and psychologically. Humans aren't meant to be socially isolated.
How much of this went on was highly variable by state and county (sometimes even municipality). In some places, restaurants closed or became takeout only. In other places, they stayed open, but had to close any buffets. Schools and libraries closed or not different amounts of time in different places. Different universities took different degrees of action and distancing for different durations. Every single chain of stores took different measures (other than hanging up signs re-iterating whatever the state department of health said).
The differences were highly variable. I have family in rural areas whose lives changed not one iota unless they had to travel for business to more urban areas. I have more urban people in my circle who were locked into their residence almost all the time, working and school from home. And then, there are the grocery store, food delivery, and health workers, who were working until they dropped, short staffed, in a sea of anxiety, many getting Covid multiple times.
There was no single experience of lockdown status even within just the USA, let alone across countries.
half my friends lost their jobs because of the not-a-lockdown. The fact that we could still buy FOOD doesn't mean we weren't locked down. What a terrible take.
Well guys, we weren't physically barred in our homes and starved so we weren't locked down. Brilliant.
I upvoted you because I agree with the essence of what you write. The problem is admittedly the enormous geographic variability of the measures that were adopted. None of us is quite sure if the debate is focusing on measures of Elbonia or rather those of Santa Banana.
Well then lets apply the same standard to the statement that there were no lockdowns. Some countries like New Zealand wouldn't even let their own citizens fly home, and there were stories about people in China having their doors nailed shut by the police. You don't get to make a blanket statement that, "there were no lockdowns" and then downvote everyone that replies because they weren't specific enough.
Yes, if the guy writing that is in one of those countries with lockdowns. But if he's in say Switzerland, he's not exactly wrong. Listen I'm not going to defend intellectually dishonest people either but I'd invite him to clarify which country.
> Besides the economic harm and potential developmental harm induced by closing schools for kids, I think lockdowns did incalculable social harm to society.
Don't confuse correlation with causality.
You had politicians abusing the covid pandemic with accusations of being a made-up conspiracy and in the process enticing hatred towards health officials who enacted standard public health policies, to the point that hardline militants even attacked them for suggesting that people should wash their hands.
After over a year of this blend of propaganda permeating society, of course you'll have the most vulnerable segment of society, overly represented by the undereducated, building up an uneducated grudge against society in general and in particular against "the system", whatever they were told to believe that might be.
It gave huge swaths of the population a grudge against the system, a chip on their shoulder that won't go away anytime soon.
It gave belligerent jackasses as stage upon which to perform. I suspect the grudge was long there, and the chip sat so long on their shoulder prior to the pandemic that it left a stain on many of their shirts. We should not cater to them.
It burned up goodwill and trust for experts and politicians (who generally didn't have much to spare in the first place.)
Again, just an excuse. Throwing the baby out with the bathwater because people that know far more about the subject than you do got a few things wrong, well, that's just being immature and/or supporting a narrative. We should not cater to them, either.
But at least we can agree that closing the schools was a bad idea.
The US government estimated that the asian flu pandemic had a CFR (case fatality rate) in the American population of 0.1 %. [1] The US government estimated that Covid-19 had a CFR in the american population of 1%. [2]
So Covid was only ten times deadlier. But certainly we should have had the same response. Those "libertarian" organizations are getting less and less veiled about their hatred of humanity. Sometimes I wonder if they are some extra-terrestrial cockroaches in human shells out of Philip K. Dick story out to wipe out all humans.
Note that the above is understating things because the 1% Covid CFR number is dilluted by a lot of later covid cases when people were vaccinated and the later less potent virus strains were out. In the beginning with the original strain and the deadly delta strain and no vaccines Covid was much deadlier than that 1% number.
I think the lockdowns are a mixed bag, yes many people didnt die from COVID because of them - but many (smaller number) people did die of things not COVID from them.
I still think on a numbers perspective that the lockdowns saved more lives than not locking down would have - but it does not help the cause of "keeping that tool in the public health toolbox" to not acknowledge the externalities of its face - its not a completely benign policy without externalities - its just significantly less bad than the alternatives.
I think we should study this more, to try to form a consensus when a lockdown is appropriate. I think a COVID scale illness is, but when does that cease to be true? half of one? 3/4? who knows, we've not spent much time thinking about it yet.
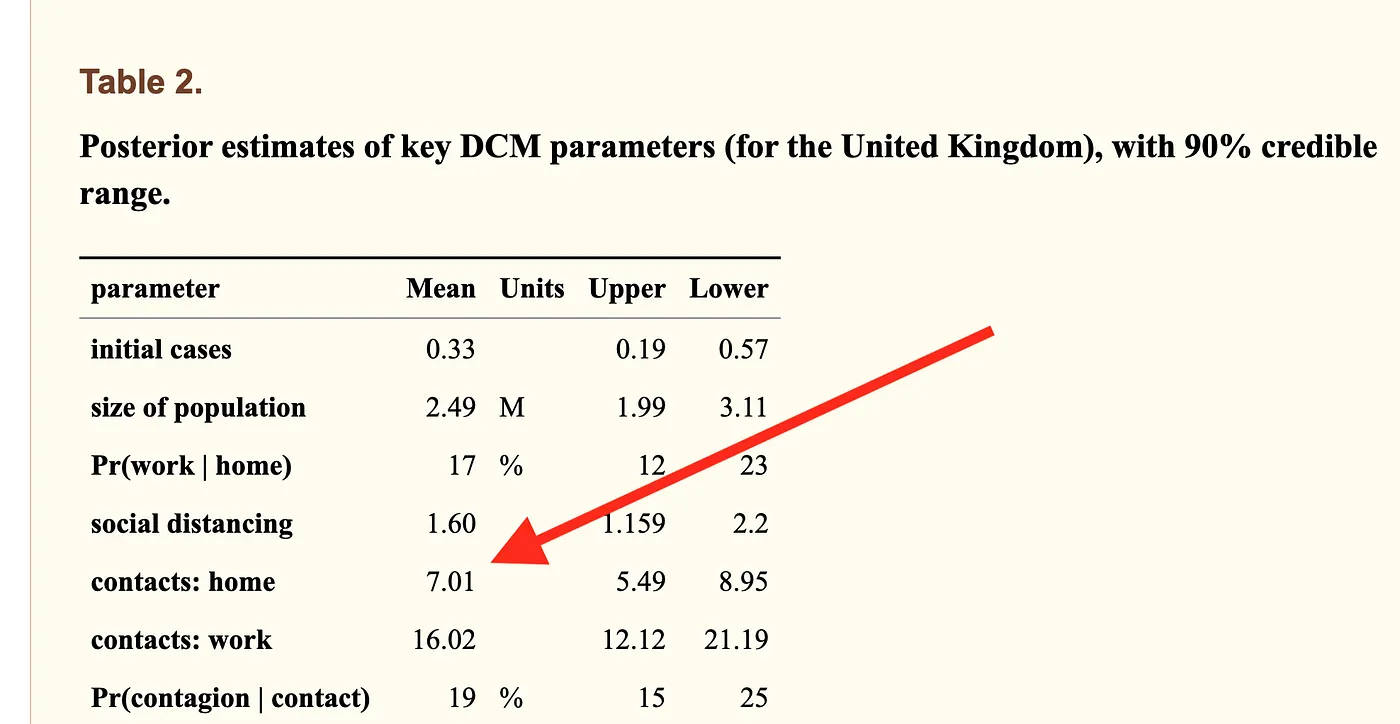{kind=link}
{kind=link}
The point of the lockdown was not to entirely stop the spread- that was obviously not happening. It was to slow the spread to avoid overwhelming hospitals.
It allowed us to reduce the lethality of COVID-19 by having more resources per sick person.