MD and I work in the field. The technology is called CAR-T, as the article mentioned. It’s been used pretty widely for “liquid” tumors for a while (eg leukemia, lymphoma, and multiple myeloma),but solid tumors are particularly difficult to target using current CAR-T therapy. If this CRISPR tech can be applied widespread to solid tumors that opens up a huge swath of patients that can be treated.
However cost and logistics are a huge factor. CAR-T therapy currently cost about $300,000-$500,000 to treat a patient. Beyond the cost of the immunotherapy you require a huge institutional investment because there are characteristic side effects that occur within the first 30 days of treatment which necessitates patients to be either admitted to the hospital for 30 days or stay in close proximity with daily check-ins (yes the cancer is getting treated BUT now your immune system is hyperactive which can be very dangerous in the short term).
Very few academic hospitals, let alone community hospitals, have this bandwidth which will lead to cancer care being concentrated in a handful of a few very large cancer specific institutions.
This isn't CAR-T, which is a chimeric antigen receptor (antibody) grafted onto a T cell. This is a T cell with an edited TCR receptor. This is quite different and comes under the 'adoptive TIL' category of treatments. It allows targeting of antigens not displayed on the cell surface. Every cell has to process their protein through a proteasome and present those peptides on the cell surface, which is where the advantage of this type of treatment comes in. In CAR-T we target a surface protein, and there's nothing to stop the cancer removing that protein from the cell surface.
I received conventional, pre-CAR-T treatment for ALL Leukemia about 9 years ago. That consisted of chemo, total body irradiation and a successful bone marrow transplant. Cost was $300,000.
OP is talking about CAR-T therapy which is in routine clinical practice. In the UK costs have gone from £600k to around £250K That includes the surrounding medical, nursing and follow up care. In the US costs are likely to be more than that.
The article is talking about a very bespoke process where they take a patient's cancer, sequence the whole thing, select mutations they think will be presented on MHC-1, predict the antigens visible, and 'somehow' (I need to read the article more carefully to figure out how they did this) select a TCR sequence which will bind to that. Then they use CRISPR to graft that onto the TCR gene of a T cell from the patient (3 types by the looks of it), and re-infuse the targeted cells.
I responded to another post similar down but you are correct. The drug is $500k, the surrounding medical care / hospitalizations etc pushes the total cost to over $1,000,000
Independently of where one stands politically, we Swedes are lucky that our government can import expensive medical treatments from large evil US corporations that do the work for us.
Its not like US is the only manufacturer of medical tools which and treatments for the only way to pay is via that ridiculous medical system they have there. Thats a nice fable that US pharma would like you to believe since they profit from it generously.
Those items are done all around the world, ie in Switzerland. And a lot of tools come from ie Germany (Siemens), Netherlands (Philips) etc.
I chuckled when I read this, because when I think about the "brand" for Philips/Siemens, my default assumption is "American company". When you mentioned it, I recalled "Oh yeah, I've heard that Siemens is german before", but being raised with the "American Exceptionalism" mental framework means this thought isn't the default. (Versus brands like Volkswagen/Ikea/Toyota).
Embarrassing example: I was watching Federer play Nadal and thought "Wow, American athletes are great. I'm proud that we have the best. Wait... neither of these guys are american. Let me google where they're from. What am I so proud of exactly??"
The number of times we hear "this is the greatest country in the world" on a daily basis is really quite sad.
I’m sitting here in America, literally half a mile from one of Philips major research facilities. I know folks who work there - although many are Indian grad students.
Not sure how the whole “German” thing is relevant.
I live near a big tech campus and am surrounded by foreign firms who do massive amounts of R&D in my neighborhood.
I am not trying to come across as patronizing, but the US is, in my opinion, the greatest country in the history of the world.
I am sorry that you feel that way about your country as a fellow human (I am not being sarcastic), but my positive view on American exceptionalism has nothing to do with you personally, just your culture.
If you re-read my comment and the comment I was replying to, you will see that I wasn't making any claims about America being or not being the greatest country in the world. I was pointing out how "American Exceptiolism" will sometimes cause me to think things which "are great" as being american when they aren't american at all.
* you: Swedes can import expensive treatments from US corporations
* Parent: Alot of those are from non-US (Switzerland, Germany, Philips)
* my comment: When I think of "Philips", I think it's an american company
* my comment: When I was watching 2 top athletes, my default assumption was that they were american, even though it's extremely obvious that they aren't. Which exposes how ridiculous the framing is.
Unless a company actively promotes that it’s a foreign company in their branding, “German engineering”/“Swedish design” or similar with their name/branding, I will assume it’s an American company.
I think one of the reasons "American Exceptionalism" is dangerous, is that it holds us back from improving on things which aren't actually the best. If an American politican says "This is the greatest country in the world", that is an emotional argument to keep things exactly the same.
The US has for 70 years enjoyed the distinction of being the most powerful country in the world by various reasonable metrics, almost certainly the most powerful to have ever existed. But is it the greatest country in the history of the world? Depends on what you mean by "great". We've undertaken atrocities; started wars; destabilized entire regions. Despite being unbelievably rich we have people dying to treatable illnesses like diabetes for lack of medical care. We face more violent crime than other comparably rich nations, and whole swathes of non-white individuals have valid reasons to fear the very police force that should serve a protecting role. Despite being in certain respects undereducated, we saddle those who seek higher education with enormous debt burden. I could go on and on.
I'm not saying that other nations haven't done things worth vehemently criticizing, but it seems a bit ... gauche to call the US the greatest country in history full stop.
One metric, in fact the only metric for me as father of 2 small children currently is: where do I want to raise my kids, to have the best environment to grow up, to be happy, know true freedom and have these qualities transfer also into adult life?
Despite all its qualities and uniqueness, objectively US wouldn't rank in first 10.
Americans are often embarrassed of America, which I think tends to stem from the fact that they think it can be even better than it is. Which isn’t a bad way of looking at things, IMHO.
The US is of course not the source of all the tools. But the ability to charge Americans high prices for novel treatments make the US the dominant source of funding for clinical and pre-clinical medical research, whether or not those funds flow into German tooling.
yes, in the Democratic People's Republic of Germany (specifically in the anarchist Berlin enclave), a friend of mine received successful cancer treatment that ended up costing well over 500k (and she is not even German)
Private, though you don't pay it out of pocket for 95% of stuff as the medical aid covers it using your premium. Public is probably much much cheaper (free) but not a place any sane middle class person here would ever want to experience.
And the first sequencing of the human genome took 10 years and cost hundreds of millions of dollars. Today you can do it for $100 in a couple of hours.
Does that $300,000-$500,000 go mainly to super-highly qualified labour, expensive materials or rare machine time? Still more or less on par with a few rounds of chemo.
Good question and I should have been more clear. The drug itself is $300,000-$500,000. It’s crazy expensive, but it’s not like a hedge fund patenting 100 year old insulin or something, it’s a bespoke medication. I still think they are price gouging however.
The medical care would likely add another $500,000.
There were some drama in England about NICE not willing to put the medication on NHS formulary because of the sheer expense. Is it better to treat 1000 diabetics or one cancer patient?
To put this in perspective, a family member was treated for leukemia and our billed* medical expenses hit $300,000 in the first 2 weeks of treatment. This included the initial hospitalization, attempted install of PIC line, install of broviac catheer. And secondary hospitalization in hepa controlled room due to other illness during an immuno compromised period.
The standard treatment continues for ~2.5 years so this was only a small portion of the bills we received.
*obviously what is paid by insurance + out of pocket is very different, but that level of billing is insane. Also you really don't want to be fighting insurance and the medical center over billing while your family is undergoing cancer treatment.
Well what makes the drug so expensive? Is it mostly mark-up for a high risk venture, is it actually taking 2+ man-years to formulate the drug for a particular patient, does it require already expensive components/reactants/whatever, bespoke machinery that would only produce a few doses in its lifetime, or some combination thereof?
Not responding with regard to any specific treatment, rather more generally.
It’s a mixture of several things:
* New/Niche Equipment
* Few few commoditized inputs (e.g. lentiviral vector)
* Labor Intensive
* These setups look more like labs than large continuous or batch manufacturing sites
* Everything requires GMP
* This can mean weeks of training new personnel (even for well known manufactures)
* Additional time & resources for FDA approval (safety testing, documentation, validation,
Part of the NICE discussions is to apply pressure to get a lower price. I feel like this is a good thing to prevent gouging. The second version of the Cancer Drugs Fund is also useful here, because it makes available stuff that isn't in the BNF.
My question would be more like, what would be needed for it to fall to 10% of its price ? Still only limited to developed world, but at least would make it more accessible
It might reduce prices, but I wouldn't trust pharma companies to put safety over profit. We've seen time and time again that pharma companies will do the bare minimum to prove safety, which has lead to a large amount of harm (see Vioxx, Thalidomide, etc). I don't think reducing what safety measures they have to prove will make therapies safer.
The study on medical devices indicates that safety actually improves with deregulation, due to the combination of a larger market and litigation.
In any case it's obvious to me at least that in the long run, if medicine sees the same pace of innovation that, say, smartphones have seen, or even that the cosmetic surgery field has seen, we would have much safer medical products and services just by virtue of them being significantly more sophisticated, less invasive etc.
Finally - even if all this weren't true - without price reductions, it will be increasingly the case that the safest and most effective treatments will be out of reach of the masses, due to simple economics/scarcity. I would rather have some lower quality products/services available to the public, and the best quality ones be more accessible, than remove the lower quality offerings but also deprive the public of the best quality ones.
>>Appropriate regulation, not deregulation, is the name of the game.
Based on what case studies of industries? Look at the prices in the most regulated sectors. In medicine, it makes the most effective treatments inaccessible to the wider public, with innovation that reduces costs progressing at a glacial pace.
Medsafe regulates medicines, what is effective, and Pharmac buys them, for the whole country.
Pharmac drives hard bargains with pharmaceutical companies. There is a lot of money to be made (even in a small market like New Zealand) if a medicine is -bought (read subsidised) by Pharmac.
The effective treatments are available. The highly experimental, might work, might not, might kill you, might make you sicker, might cure you medicines are held at bay by medsafe, and when approved are made affordable by Pharmac.
Of course Pharmac is under constant attack by the completely unethical pharmaceutical industry and equally unethical senior doctors - all hopelessly corrupted by the enormous sums at stake. Huge astroturfing campaigns exploiting ill people and their families. But the benefits are so huge that it has survived.
There is talk about extending the model to medical devices and consumables.
Appropriate regulation is absolutely needed because the incentives that drug companies and medical equipment manufacturers face are opposed to the incentives of the community.
Free markets, in this case, make people sick and impoverished.
>>Medsafe regulates medicines, what is effective, and Pharmac buys them, for the whole country
This is no different than what happens in the UK and you're gonna run into the same problems that the UK has where cutting edge treatments cost too much for the government healthcare program to cover them.
The problem in medicine is that innovation is too expensive, and too slow to rollout, and this applies just as much to New Zealand as anywhere else.
Cancer and heart disease should have been cured by now, considering the pace of innovation we know is possible.
>>medicines are held at bay by medsafe, and when approved are made affordable by Pharmac
You can't legislate affordable cutting edge treatments into being. Pharmaceuticals have to be incentivized to spend vast sums on developing them, and a mechanism needs to exist to select the best amongst those treatments for further development.
Evidently, that selection and resource allocation role is best left to consumers and their doctors, as opposed to one centralized body.
>>Appropriate regulation is absolutely needed because the incentives that drug companies and medical equipment manufacturers face are opposed to the incentives of the community.
Their incentives are to be selected by consumers, and the best way to do that in medicine, like any other industry, is to produce high quality products at low cost.
See the study on the positive effects of down-regulating medical devices, which are lower prices and greater safety.
>>Free markets, in this case, make people sick and impoverished.
Why this choice? In the case that a treatment is life-saving the ethics board can approve experimental treatments on a case-by-case basis. Medical laws just don't allow patients to make this choice for themselves.
The problem with the centralization (regulation) approach is that it assumes one body can be chosen that will be optimal at risk assessment. In practice, the process of developing good risk analysis frameworks - that strike the right balance between cost, risk and efficacy - is often best discovered through trial and error, and that requires the freedom to try new products in the market.
There's an ethics board per hospital. And there's different countries. You can in fact shop around if that's what you want to do. You can do this, both as a patient and as a pharmaceutical company. It's just really expensive.
Even a law requiring an ethics board, with statutory requirements for how that ethics board is constituted, is a one-size-fits all meta-solution, created by one body: the national regulator.
I'd be curious to see what would happen if reasonable regulations stayed in place but we capped/removed the risk associated with litigation (assuming regulations were followed). I.e. what portion of "adhering to regulation" is reducing the speed of advancement because of fear of litigation, as opposed to just the cost of sticking to the regulation.
Seriously, innovation needs to be encouraged and all the gates hamper that. But being critical of the medical cartel gets flagged/downvoted quickly here. See comment higher up.
US-based pharmaceutical companies maximise their margins in the US to make up for smaller margins in other markets. In many other countries, most prescription drugs are purchased by the government, which gives the government a lot of bargaining power which it uses to drive margins down. Prescription drug purchasing is much more disjointed in the US (negotiating with many private insurers instead of just the government), giving more bargaining power to the vendors and supporting higher margins.
This doesn’t make sense. Consider two scenarios: company ABC sells only in the USA and Company XYZ is otherwise identical but also sells to Asia.
You are implying that because XYZ has lower profit as a percentage yet higher profit as a nominal dollar amount, that XYZ will charge its American patients more. My intuition says both ABC and XYZ will charge Americans the same, namely the highest amount it possibly can under market/regulatory/PR/competitive considerations.
The same that happens in medicine happens in college textbooks - and other forms of high margin, but relatively fixed/finite initial investment and stable cost to produce.
American scholars write some of the most respected textbooks in the world, they are then sold in US colleges for $100-400/each. The same book is then sold in SE Asia and Africa for $10-40/each.
The madness of the US healthcare aside, CAR-T is really a somewhat complicated therapy. There are no economies of scale there, unlike in pills. Each patient requires a lot of painstaking work that can only be done on specialized machines by highly qualified people, plus the safety requirements are really high.
Activating the immune system is risky. It is strong and it can crush cancer in mere weeks, but it is also very dangerous to friend and foe alike. Basically, you gather a lot of absolutely ruthless and stupid troops and tell them "here is ze Flammenwerfer, burn the enemy to crisp, but don't destroy anything else".
I sadly know little about all this technology.
It is fantastically expensive at the moment from what you say.
That keeps it away from the vast majority of cancer patients in the world.
Technology does tend to get cheaper over time, though not always.
Do you think this treatment could reach $30.000 in 2,5,10,15 years?
And $300 in another 10,20,50 more years?
I've watched the prices of patented drugs quadruple in less than 5 years, to the point where a 30 day prescription can cost thousands of dollars despite the same medication costing $40 in countries like the UK. Drug companies have absolutely no reason to drive down prices of the patented treatments they have a literal monopoly on.
As with many medical drugs, the marginal cost of production of the medication is small, but it is dwarfed by the cost of research, trial conduction and FDA approval and is patented. Additionally for CAR-T there is rather intense post-adminitsation care required.
For the pharma research companies to be profitable, they need to recoup the above costs on the limited number of cancer patients there are.
For a widely applicable technology like CAR-T, if you can figure out how to distribute the costs over multiple types of cancers, you could have a much larger pool of patients to distribute the cost over, such that the marginal cost of production is a more meaningful component of the cost to patient/insurer.
Pharma typically spends a lot more on marketing than research. In fact, there is little to no correlation between research costs and the cost of a drug.
There are companies doing research in applying CAR-T for treating animals. This has a much easier approval process since it is run through USDA and not FDA. I'd expect to see faster advancements in treatment and lowering costs and then having this tech brought over to humans later.
Although I'm hesitant to make strong statements because inflation plays a significant role here, cars are much more sophisticated than they used to be but also very expensive as a result.
In 1916 a barebones model-T cost $360 [1]. That's $8400 in 2019 dollars, and $9800 in 2022 dollars. This is actually what led to the normalization of planned obsolescence. [2] The widespread availability of reliable and cheap vehicles posed a problem for manufacturers which had, to that date, primarily just competed on quality and price.
What do do when you can't create something more cheaply, or of a higher quality? Curve some edges, strap a layer of chrome on it, and market it endlessly to get people to buy the fundamentally identical product over and over and over again. Progress!
"Oh god, I can't believe you're still driving a 1916 - that's soooo last year."
> In 1916 a barebones model-T cost $360 [1]. That's $8400 in 2019 dollars, and $9800 in 2022 dollars.
Not too much like a modern car to compare, though. Still no electric starting, and not a lot of capacity, creature comforts, or speed. Time between major overhauls was ~15,000 miles. Overall lifespan of the car was estimated as 100,000.
> What do do when you can't create something more cheaply, or of a higher quality? Curve some edges, strap a layer of chrome on it, and market it endlessly to get people to buy the fundamentally identical product over and over and over again. Progress!
When we're comparing to vehicles with anything like modern speeds and capacities,... average vehicle age / longevity is higher than its ever been. (It's a bit more difficult to compare before the mid-1960s because vehicles were rebuilt and overhauled so much before then...)
I don't think technology improving over long time scales runs contrary to the nature of the question, or answers it. The first computer, the ENIAC, required a small building of space, cost about $6 million, and ran at around 500 FLOPs. Today a modern GPU is several inches long, costs a couple of hundred dollars for a pretty decent one, uses minimal electricity, and will run literally tens of billions times faster than the ENIAC.
Well, overall hedonistic adjustments to price are complicated and controversial.
I'm just saying: there's not really any cars like a model T anymore. Not just because of increased technology, but because of improved underlying technology: customers expect more (volume, mass capacity, interior comforts, ancillary features, speed, etc) and that increases cost.
We could probably make something a lot like a model T pretty cheaply still, if there were a big market for it.
I think that depends on what you classify as "extremely cheap". The cheapest car in the U.S. market is the Spark at under $14k, but it's been discontinued. The Versa and Mirage both start around $16k.
I'm unaware of anything else under $20k, although the Ford Maverick is impressively reasonable at $21k.
Phone cameras have improved phenomenally and are great webcams. You can even clip them to your laptop if needed.
For webcams we now also have eye/head/movement tracking, automatic background insertion, and other improvements (as well as added features like turning you into an animated cartoon character) although arguably those are from webcam software rather than hardware (though there are examples like the Apple Studio Display webcam which uses their neural engine hardware.)
I'm sure the launch costs (which can be worked into $/kg for payload) can be easily looked up, and show that SpaceX's reused rockets are much cheaper than what came before.
We haven't seen a reduction in space insurance premiums of any particularly large magnitude which I would expect if the costs of launching satellites into space had been substantially reduced.
General aviation is quite a ways behind where cars are right now. There are new planes like the Cirrus SR22 that have made advances, but they are far from ubiquitous. Most GA planes are like driving a 57 Chevy except if the engine dies, you die.
Those fancy digital glass cockpit avionics in the modern versions are not cheap. On the other hand, those ancient mechanical avionics were crazily expensive, too.
Same model from the 70s with the same avionics in 2022? I'm not sure that's even available. C172 entry model is full glass today. Interior looks a lot more shiny, too.
Maybe not same model but actually same plane? If it was new in the 70s it is used and much cheaper now. If it was new in the 50s, the used price in the 70s might have been lower than it is today though. That's caused by the minimum price the market defines for anything that's airworthy.
Maybe that's an investment stragtegy, buying used planes when they reach their minimum price, then keeping them, flying minimal hours to keep the engine alive, to sell 50 years later. But any potential gain will be neglected by hangar and maintenance cost.
Obviously not op, but it sounds like the issue is that the cure makes you sick in the short term which requires expensive care. If the sickness is inherent to the solution it’s hard to see how this gets cheaper.
The next generation CAR-T treatments are supposed to be "easier" on the immune system and hopefully don't require the prolonged hospitalizations. But that is 5-10 years away.
Cancer won't be a problem by 2027, at least for the people who don't already have cancer. By 2030 there will be drugs that can even cure stage 4 cancer with next to nothing side effects. (AI and some form of quantum computing will help find these drugs)
Researcher working in a related field. The above is just patently false. There are currently no drugs that can do this in lab-animals, let alone make it through clinical trials in time by 2027.
Computation is also not the bottleneck of research, it's the amount of training data, see ICGC https://dcc.icgc.org for the current state of the art.
Remember that each tumor has 3 billion base pairs (A,C,G,T), each of which can be duplicated, deleted, mutated. It can also be affected by methylation. Expression of the genes comprised by these base pairs is also affected by the micro-environment of the cell. Any machine learning model will have far to many parameters for far to few observations, to pick the rare drug that can cure stage 4 cancer (assuming it even exists) out of millions of possible chemical compounds.
From what OP said, I doubt they'd be able to keep up with the additional load of patient care (admittance especially) so there could be long wait times.
At some point, capabilities like this mature on the science end but are slowed down on technology (scaled manufacturing). That would take significant investment by a big pharma or a new venture-backed investment to go after things like this. Fingers cross this happens within my lifetime.
From the article:
>“This is a tremendously complicated manufacturing process,” says Joseph Fraietta, who designs T-cell cancer therapies at the University of Pennsylvania in Philadelphia. In some cases, the entire procedure took more than a year.
There are clinical trials on Glioblastoma CAR-T treatment but it faces the same problems as any other solid tumor - namely the solid tumor microenvironment is not amenable to the current generation of CAR-T treatments
In addition one of the dreaded side effects of CAR-T is neurotoxicity. CAR-T can cross the blood-brain barrier and leads to inflammation in the brain. You can treat it pretty quick with steroids but this side effect along with several other pro-inflammatory ones is the reason for the 30 day hospitalization sp treatment.
Not CAR-T or CRISPR AFAIK, but there's been some recent breakthroughs with getting treatments past the blood brain barrier, and promising glioblastoma treatments are in the pipeline as well. This is just what I've seen on the internet news, you'd find more than I know about it with some internet searches.
I hope you aren't affected by GBM. If you are, or someone you know is, my only advice is to live life to the fullest while you can and don't let yourself fall into denial of the prognosis.
Not me but my wife. Will just put this out there for anyone else, the advancements made in Cancer treatment in the past few years are impressive. Don't lose hope.
Also, listen to your doctors as all of the sudden everyone is oncologist. Listen to your doctors, seek second opinions, do research but question everything as there is a lot of snake oil for sale.
I'm so sorry. My mom was diagnosed a few years ago and she got preyed on by snake oil salesmen to the tune of 6 digits. The money doesn't matter to me, but people are really fucked up.
I can recommend Duke's neuro-oncology center though. They did a great job with her when Sloan Kettering wouldn't touch her.
Best of luck to the both of you and hang in there.
All of you AI people reading this should work on predicting side effects and outcomes from these therapies. That would help decrease the cost tremendously.
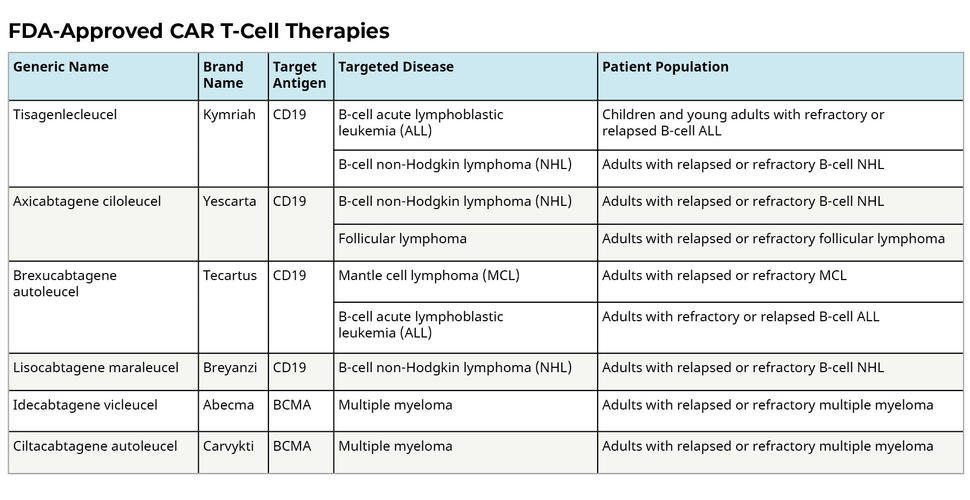
You'll want to sign them up for a clinical trial. Only CAR-T cell therapies that are FDA approved are for leukemias. [ and as a commentator points out, for lymphomas, I had always thought lymphomas were a subset of leukemia. mea culpa ]
Took my wife to MSK for a second opinion on the treatment plan for her ovarian cancer. They were beyond useless. They wouldn’t say or recommend anything until the current treatment plan (eg round of chemo or surgery) was complete, yet it was incredibly difficult to arrange time with them to review results when that time came.
Basically we got nothing from them.
Not sure what my point is other than if you’re getting a second opinion, discuss how the provider will integrate their assessment with the existing treatment plan. And at the end of the day it’s the doctors and nurses you get that make the difference in your care, not the building.
Thank you. We visited Cleveland Clinic as well and received very similar results. I briefly thought about starting a class for cancer patients to help them navigate the medical system in the US. I had to try to learn to fly from the front seat of the plane and it was a bad experience.
She passed in 2020, just two years after diagnosis.
> On 1 April 2022, the FDA approved axicabtagene ciloleucel for adults with large B-cell lymphoma (LBCL) that is refractory to first-line chemoimmunotherapy or relapses within twelve months of first-line chemoimmunotherapy.
I was in a clinical trial, though, but that was to determine the effectiveness of Anakinra in preventing serious side-effects; in my case, I only got a few mild fevers, which is the biochemical equivalent of winning the lottery, in a lottery where losers end up comatose and intubated.
I am very happy for your outcome, can't imagine the stress and fear you felt. So glad you had success, let's hope this becomes commonplace and people are saved from such a wretched fate.
I'm also very happy, especially since I was in complete remission as per a PET/CT scan a month after infusion after my cancer had survived two previous lines of chemotherapy (DA-EPOCH-R and R-GemOx) and had even shrunk but became more metabolically active after the second line. I'm still in complete remission, with further destruction of the tumor, six months after infusion, and there's some evidence the CAR T-cells can persist a decade after infusion:
Ahhh, personalised treatment for the mega rich. Soon our billionaire gods will be able to live far beyond a normal lifespan. I wonder how this will impact society?
Only tangentially my field, but both cytotoxic and helper T-cells bind on antigens, and indeed this work CRISPR edited anything with a TCR to their (3) preferred, cancer-targeting receptors (for each patient).
Your CD4 T cells are basically the directors of your immune system. They license CD8 T cells (T killer cells), B cells and recruit NK and immune cells to sites. The type thought to be most anti-cancer are the Th1, which recruit CD8 T cells and NKs, and are optimised for intracellular pathogens. Cancer can be thought of as an intracellular pathogen because it harbors mutations.
> 1) Being able to rapidly sequence the genomes of cancer cells to detect common mutations
Only of the cancer cells? How are mutations detected in the 0.4% of the DNA that differs in different human beings? Can't there be non-cancerous changes in the other 99.6% that are present in all cells? Is it just a matter of cost, sequencing both too expensive?
The article mentions: "...sequencing DNA from blood samples and tumour biopsies, to look for mutations that are found in the tumour but not in the blood."
This is pretty common for most cancer genotyping tests. (Sometimes they compare tumor with saliva or some other "benign" source, but the principle is the same.)
It’s good progress but I want to say it’s still not a magical cure - the fundamental idea is flawed - the tumor can and likely will in many patients just mutate the immunogenic epitope.
I haven't seen evidence of cancers re-mutating mutations. They tend to develop new mutations (as in the clonal evolution hypothesis), and they can completely change their cell surface expression. But I suspect that they are unlikely to mutate an already mutated gene.
I guess for the treatment to be most effective you need to target some of the earlier mutations, rather than a small clone.
From my perspective, and not having read the paper, I thought the technology to predict what TCR would bind a particular peptide on a particular MHC-1 was not there yet.
Cancers have higher mutation rates and also constantly rearrange their genome including deletions. Given that they’re looking for Novel epitopes it goes to reason these are not high copy number hence deletions can also remove them fully. It’ll be hard for me to believe that a mutagenic cancer (which is a given here since you’re looking to treat cancers with actual mutations) will not eventually gain resistance to this therapy.
Yes you are right, I should have said that re-mutation of mutations happen far less often than accumulation of additional mutations.
Novel epitopes should be high copy number - and driver mutations will be present in 80-100% of the cancer cells. It depends how many cancer cells you get in your biopsy that you sequence I guess.
It is easier for a cancer cell to mutate or remove a cell surface protein than to mutate the same mutation targeted, but you are right - that can happen and I'm sure will be a form of treatment resistance for these types of treatment in the future.
> But I suspect that they are unlikely to mutate an already mutated gene
Could you elaborate? I'd like to understand what you mean, as I don't work on onc. Aren't recurring mutations in response to treatment in f.e EGFR is the reason we keep developing multiple generations of small molecule therapies for it?
Yes, I didn't mean impossible, I just mean compared to accumulating new mutations elsewhere, and compared to downregulating surface proteins (which can be the issue in CAR-T).
Do you know of any journal articles that cover step 3? I'm very interested in how this whole process works and can't seem to find much (paywalled at Nature for this one.)
I'm a haematologist who is involved with patients who have CAR-T (I don't do it myself, but do other types of transplant and I look after the patients before and after) and my research area is in the way T cells target cancer.
This study isn't CAR-T. It is more similar to adoptive TIL therapy because it is using the T cell receptor (TCR) to target the cancer's mutations. This has a huge advantage over CAR-T.
At the moment we use CAR-T to target, mostly, B cell cancers. These cancers have CD19 and CD20 on their cell surface, as do most B cells. We can safely target these cells because it turns out your B cells aren't critical for life. Think of it like an amputation. Your B cells went rogue, you wipe them out.
The problem is this doesn't translate to other cancers, which don't have an obvious cell protein you can target specific to a group of cells you can do without.
All cancer cells have mutations, and all cells in the human body have to display a sample of its proteins on its cell surface. This way our immune system regularly identifies cancer and removes it. Cancers that get established have somehow leveraged local immunosuppression to hold off the immune system, and so the immune system and cancer become a stalemate, or worse the cancer takes off and kills the person.
If we can target the mutations of the cancer, then we can get at the heart of the cancer itself.
You might ask why the cancer just doesn't display it's antigens on the surface. If a cell does this it gets removed by NK cells (natural killers) - our body's fail safe.
What I find interesting is that I didn't think we were close to predicting what TCRs can bind to to a peptide on MHC on the cell surface. I'm going to need to look at the article to findout how they did this. I suspect they used a library of known TCR-antigen interactions.
Since there are people here that seem to know a bit about this stuff, I will take the chance to ask some naive questions ;)
Do I have this right that CAR T-cells have this engineered B-cell/antibody like receptor that recognizes antigens only on the cell membrane. While the regular T-cell receptor can look into cells as well? And that's why the T-cell receptor is potentially better at recognizing solid cancers?
So cancers usually create this immunosuppresive environment, wouldn't this stop this engineered T-cells as well?
Yes, CAR-Ts are really a B cell receptor (otherwise known as an antibody) grafted onto a T cell. Antibody directly binds things like proteins, and usually targeted to things found on cell membranes.
Also on the cell membrane is MHC-1, which shows a short (9-11 amino acid) fragment of protein produced from inside the cell. Our T cells are trained in our T cell kindergarten (the thymus) to not identify our usual self proteins, but detects anything different. They have already been demonstrated to identify single amino acid changes from normal.
Yes, the micro-environment means the immune cells reach a dynamic equibrium. This is because when a cancer presents to healthcare, it is already a chronic process. The T cells are termed 'exhausted', but it's debatable whether this is a good term for it, because they are still active.
A lot of cancer treatment 'shakes up' the microenvironment. This can be enough to tip into a cure. When you make CAR-Ts and adoptive TILS you either pick healthy T cells not involved in the cancer or buff them up in the lab, both in numbers and health.
The hope is that a refreshed army of T cells will push that dynamic equilibrium towards a cure.
I think there is more information than that. There are 20 amino acids, so around 1x10^13 possible sequences.
This is also a clue as to why we don't have a perfectly rigid system, as a library of T cells capable of recognising every combination would weigh 600+ kg.
I had a brain fart. I was thinking of DNA base pairs not amino acids :) Thanks for that.
There are 20 amino acids. Each AA in a sequence represents approx 4.3 bits. So 9-11 AA would be 38.7-47.3 bits. Not quite as much as an MD5 hash (128 bits), but still quite a bit of info.
My 27 year old sister got CAR-T for leukemia earlier this year after a failed stem cell transplant. She's in remission. It's incredible, literally curing cancer.
If you don't mind me asking, how was her pain for the 30-days after period? Another poster said they were extremely lucky to only have suffered a few fevers but some people were in a coma.
As per the article, calling this a "success" is a little over the top. Out of 16 patients, it stopped progression of tumour in 5 had stopped but it doesn't say it decreased.
Moreover for 2, it had adverse reactions when admittedly the dosage was low. I won't call that a success. IT is a good start and promising result. "Success" would mean at least 50% patients REDUCED the tumour. So let us not hold our breath yet
Is the end state of this to eventually modify people's bone marrow to produce modified T cells, or do they envision treating people with infusions of modified T cells? On one hand, permanently modifying people's immune systems seams fraught with challenges. On the other, a steady supply of cancer killing T cells sounds like a strong protection against recurrence.
This is an ongoing discussion in CAR-T. At the moment we only have 'autologous' CAR-T, which means they are manufactured from our own cells. The big advantage to 'allogeneic' CAR-T is that we don't have to take the time (several weeks) to modify T cells for adminstration, during which patients can die of the disease. 'Off the shelf' would be preferable, but there are lots of problems with trying to use someone else's T cells for the job.
The main issue is that our immune system is very good at removing non-self, so a lot of work would need to go into stopping the immune system doing this.
The article isn't talking about CAR-T though, rather TCR-modified T cells. These are very patient-specific because we have a unique MHC signature (this is why we have to find a 'match' for a transplant recipient). Previously people have taken the T cells from the tumour site, boosted them in the lab, and re-infused with some remarkable and curative results. The outcomes in this trial weren't so great but it is novel to splice in a new TCR.
CAR T-cells are cytotoxic T-cells modified so they do not cooperate with the rest of your immune system (they do reproduce inside your body, they just don't care what your "normal" immune system thinks on the matter). They do not listen to instructions from your immune system. They are modified from your own immune system so they don't get attacked, your immune system can't tell the difference between its own cells and CAR T-cells.
They are then further modified to go looking for specific targets (they go through your body, randomly, and check for specific molecules on cell membranes), and become "cytotoxic" towards them (they fire exploding acidic "bubbles" that digest a target cell).
Needless to say, this is a very dangerous treatment (uncontrolled killer T-cells roaming around inside your body multiplying ... not hard to imagine what happens if they target normal cells) and small mistakes will kill patients. In addition to directly killing off important cells, they may can also make the immune system overactive (which in fact happened in this study to three of the patients). They have a bad reputation in research for killing off entire batches of test animals when making a small mistake in less time than you'll need to diagnose the problem and, uh, "fix" it (you're supposed to kill test animals when a treatment doesn't work so they don't suffer). This is not allowed, and has to be explained to the authorities when it does happen and has ended research careers.
Normally, or should I say ideally, after multiplying a more-or-less set number of times, they die off and are removed by the body.
So no, this does not modify the bone marrow of the patient. Not at all. It just attacks and digests specific cells inside your body and dies off.
I think the fact they rapidly multiply while killing cells, inside your body, without any form of control beyond the initial "programming" deserves a, huge, honking, warning sign somewhere in that sentence. Once they go in, they may cure cancer, they may kill you in less than an hour, they can destroy your immune system and they can have your immune system destroy you.
Just to make clear this treatment will always be in the "you'll survive next week? This treatment is too risky" class.
Don't get too excited, this is medicine right? Surgeons literally cut people open -- don't try this at home.
CAR-T these days is indicated after hugely toxic therapies like BMT have failed. Plus they understand the danger of the cytokine storm responses and are at the ready to mitigate. A successful CAR-T therapy is massively less toxic overall.
If you really want to get freaked out: CAR-T uses a modified, neutered virus to reprogram the T cells. Today that's some lentivirus, but in the 2000s when this was a new therapy, it was a modified HIV. Things get safer over time!
The end state might be a little machine inside that does all of it without specific treatment, i.e. an enhanced immune system that knows what "cancer" is.
Someone makes a copy of your consciousness, runs millions of ads by this copy until it perfectly predicts your responses to various advertising strategies. Fast forward 2 months and you are broke.
An oppressive government makes a copy of your consciousness, tortures it. Learns everything. You never know it happened.
I made it up. I like the idea of taking Biblical stories and putting them into a sci-fi setting and trying to make a believable scenario. Like black mirror meets religion. Thanks for the message!
This is very good news for the wealthy, not so much for the average Joe - it will take a lot of time for this treatment to become cheap enough to be used at scale.
When penicillin was just introduced a week's course was about $100,000 in today's money. Today its better derivatives are sometimes given away for free.
That particular problem was solved by a mold-covered cantaloupe from Peoria, Illinois.
"After a worldwide search in 1943, a mouldy cantaloupe in a Peoria, Illinois market was found to contain the best strain of mould for production using the corn steep liquor process."
Reviewing a larger section of the wiki, the Peoria cantelope certainly seems to have helped.
"On March 14, 1942, the first patient was treated for streptococcal sepsis with US-made penicillin produced by Merck & Co. Half of the total supply produced at the time was used on that one patient, Anne Miller. By June 1942, just enough US penicillin was available to treat ten patients. In July 1943, the War Production Board drew up a plan for the mass distribution of penicillin stocks to Allied troops fighting in Europe. The results of fermentation research on corn steep liquor at the NRRL allowed the United States to produce 2.3 million doses in time for the invasion of Normandy in the spring of 1944. After a worldwide search in 1943, a mouldy cantaloupe in a Peoria, Illinois market was found to contain the best strain of mould for production using the corn steep liquor process. Pfizer scientist Jasper H. Kane suggested using a deep-tank fermentation method for producing large quantities of pharmaceutical-grade penicillin. Large-scale production resulted from the development of a deep-tank fermentation plant by chemical engineer Margaret Hutchinson Rousseau. As a direct result of the war and the War Production Board, by June 1945, over 646 billion units per year were being produced."
It sure did, just pointing out that there was way more involved in engineering a cheap mass-manufacturing process than scavenging at markets. Somewhere near that section is a sentence on X-ray irradiation to induce mutations, just imagine the trial and error in that, and then these labour-intensive scaling experiments.
On the contrary, it’s a very, very good news for an average Joe. Every sufficiently advanced technology starts very expensive. Then capitalism and progress do their job, and it becomes available for masses.
The path to “make it cheaper” is generally easier than the path to “make it possible”.
Keep in mind $100 is the retail price, not the wholesale price (which is what's plotted on the above graph). I do not know what the current wholesale price is for a generic epi-pen.
My point is merely that the price is trending back down now that there's competition. And again, with insurance it's effectively free for most people - either through private insurance or medicaid.
- MRNA COVID vaccine patents weren’t open sourced or available for the third world but Cuba’s vaccine solutions are
- simple things like dental care aren’t offered in the US
I think you should replace “available for the masses” with available “to the middle classes” which may seem the same to the average HN reader but not the average inhabitant of our planet
> I think you should replace “available for the masses” with available “to the middle classes” which may seem the same to the average HN reader but not the average inhabitant of our planet
The statistics simply don't back you up, as not only do the middle classes make up the vast majority of people on the planet now, but those coming from poverty into the middle class is increasing. The much missed Hans Rosling goes through it here:
MRNA vaccines are not banned to sell in poorer countries. They are currently just too expensive for them, I suppose.
Once Moderna recoups the cost of R&D and pockets some profits, it will face the need to keep selling. With the pandemic basically over, they'll need to sell to wider markets, because they have the production capacity. They'll lower the price and try to use the economies of scale by selling large amounts.
The fact that any technological advances first become available to those who can pay a high initial price (not only in money) is pretty inevitable. If something is a runaway success, the price goes down with volume, and ideally with pressure from competition.
If you want to make something vitally important available at a low price, you have to find enough money to let the producers make some profit, or at least to recover the cost of development. If you don't, nobody will consider working on it, even if they wanted, because getting an investment would become impossible, and you can't do biotech on pocket money.
(You could of course force them work at gunpoint, but not being forced to work at gunpoint is usually even more vitally important for the health of a society.)
This should stop absolutely nobody from vaccinating.
From the article: "People face a much higher risk of developing myocarditis from Covid infection than the vaccines, according to the Department of Health and Human Services. The risk of myocarditis from Covid is 100 times higher than developing the condition after Covid vaccination, according to a recent paper in Nature Reviews Cardiology."
They weren't trying to get results, only giving a low dose to verify acceptable side effects. Wait for the larger doses to render judgement on clinical results of the treatment modality itself.
I completely agree with you. If there was even one response I would be much more optimistic. Since there is no clinical signal this is at best a proof of concept and safety.
> Although the efficacy of the treatment was low, the researchers used relatively small doses of T cells to establish the safety of the approach, says Ribas. “We just need to hit it stronger the next time,” he says.
My mom has a very serious type of Breast Cancer, Triple Negative, so this news is very encouraging. She's undergoing immunotherapy - but this looks even more promising. Thanks for posting.
They're both in vary nascent stages in terms of having a comparable dataset in my layman's understanding. Both look extremely promising, some may be better suited to different classes so that's what larger studies will hopefully help detail.
yay. I read the headline in order to be elated. Now I'll read the article to get carefully optimistic and then I'll visit the HN comment section to come crashing down.
I read an article (or watched an interview) a few years ago, where they were saying that because cancer is unique to the individual, to truly cure cancer you would have to target each cancer individually. Hence CRISPR. But they also warned that this kind of control could also be used to target individuals or groups of individuals. The example they gave of what could theoretically be possible was 'making women of a certain racial group hyper sensitive to sunlight'.
Was this hyperbole? I can't find any references to it today.
It won't be undetectable. If the changes are something no one else on earth has, it will show up. If the changes are something other people have, it will still show up when comparing with their parent's DNA.
What if the "changes" are simply optimizing someone's genetics? i.e., eliminating /fixing any genes that are bad mutations, so you get the best possible combination of genes from the parents?
Or, suppose someone really does have a beneficial mutation that naturally occurred, and isn't the product of genetic engineering. Are you going to disqualify them because neither of their parents had the mutation?
I have worked in both semiconductor manufacturing and drug discovery industries. Reliably and profitably producing 5 nm chips is an extreme engineering challenge, but- it is an engineering challenge. Drug discovery is a question of science and requires a fundamentally different mindset that semiconductor manufacturing. Human biology is much more complicated than manufacturing chips (and that is extremely complicated); drug discovery is about "unknown unknowns". Discovering a drug that has the intended effects without causing terrible adverse effects is something that some of the best-funded companies on the planet struggle with.
I've done some engineering and drug development...
Image trying to write code where you can't actually see what you wrote, where each time you compile it costs $1000 and the binary randomly is corrupted 50% of the time. And the only way to find out is to push it to prod and wait a few months for someone to call you. And every prod setup is subtly different without any documentation. That's about 100x easier than drug development.
Not in medicine, but I don't think that's true. It's very hard to understand what all the consequences are going to be when you manufacture those T cells, and you also have to figure out what to manufacture in the first place, based on experimental trial and error.
Drugs ultimately have to be converted from the lab to mass production. How is it any different, they all require research, iteration, and ultimately (hopefully) engineered mass production?
Making safe and effective medicines is a lot harder than modern chip production because the subject is humans and we have to do medicine ethically.
The pharmaceutical industry predates chiptech by quite some time, represents a fairly large market, the companies are quite technological, but the underlying problems are very different from making chips. And if trials like this succeed, that area of biotech will see billions in funding.
It's not funded as much as chips but it's also a smaller overall market.
> this can't be more complicated than producing 5 nm process chips
Chips don't randomly decide to unmake themselves: there's no active, living system you're interacting with.
The other thing that makes biology so confounding is its diversity. E.g. something that works without side effect for 100,000 people will kill 1 of them, because they were in some way different than the others.
The regulation and risk-aversion is far more impactful than the funding.
It's not entirely unwarranted regulation, but fundamentally Intel can mess up 20 batches of 5nm chips before getting it right, and nobody cares. If a CRISPR trial kills someone, it's a BIG DEAL, and could potentially set the field back by years.
There are a few interesting aspects to cancer that you might find enlightening.
First is "p53, the guardian of the genome." It has the ability to trigger apoptosis in a cancer cell, when stimulated correctly. It is usually active, and (likely) terminates most of your precancerous cells via apoptosis, the controlled cell suicide pathway.
The second thing that cancer must do is shut down the mitochondria, because they are involved in apoptosis.
An interesting thing about cancer is that it needs glucose, and lots of it because it cannot use efficient mitochondria, and instead relies on anaerobic respiration.
The last interesting thing is autophagy, starvation (of sugar) which will slow down any cancer and potentially reactivate p53, depending upon your willingness to avoid prolific glucose sources.
"central DNA-binding core domain (DBD). Contains one zinc atom and several arginine amino acids: residues 102–292. This region is responsible for binding the p53 co-repressor LMO3."
When you find a way to do so, by all means let everyone know!
Ideally please make all your technological knowledge public domain. (I hope you're a billionaire and will pay to your lab staff and for other research expenses from your pocket for a decade, or for whatever it takes.)
That is both a more difficult technical/scientific challenge and a more difficult ethical issue. This could be trialed precisely because it doesn't require gene editing an entire human body.
Money is just a form of accounting for value creation. Should people stop creating value to each other? I do not think so. People who only want to extract value of course do not want any credible accounting because then they would lose.
> This entire treatment is motivated by the urge to make money from it. The "correct" thing would be to repair the faulty genes in the cancerous cells and letting the body get rid of the tumors itself.
Do you have any hint of an idea about how to do this?
{kind=link}
{kind=link}
However cost and logistics are a huge factor. CAR-T therapy currently cost about $300,000-$500,000 to treat a patient. Beyond the cost of the immunotherapy you require a huge institutional investment because there are characteristic side effects that occur within the first 30 days of treatment which necessitates patients to be either admitted to the hospital for 30 days or stay in close proximity with daily check-ins (yes the cancer is getting treated BUT now your immune system is hyperactive which can be very dangerous in the short term).
Very few academic hospitals, let alone community hospitals, have this bandwidth which will lead to cancer care being concentrated in a handful of a few very large cancer specific institutions.