Exhibit A for why "free market healthcare" is an oxymoron.
I have yet to hear a coherent explanation for how anyone can reasonably expect for price discovery to even pretend to function in a market where the consumers can't even guess the prices until after they've already purchased and frequently couldn't reasonably be expected to refuse service even if they did believe it was overpriced.
Price discovery is indeed difficult in the current market. However, the current healthcare market is no where close to a free market.
For example, suppose you wanted to start a hospital that offered price transparency, like the Surgery Center of Oklahoma does. (1)
In thirty-five states and the District of Columbia, you'd first have to acquire a certificate-of-need (CON) from the state healthcare regulators.
In order to get certificate of need, you must prove that the community “needs” the new or expanded service, and existing providers are invited to challenge your application.
Existing hospitals typically don't want new competitors taking away their patients, so they vigorously fight to prevent new CON's from being issued.
For example, Dr. Mark Monteferrante wanted to buy a second MRI machine for his radiology practice in 2003. But it took five years and more than $175,000 in fees to get the certificate. (2)
And conlaws are just one example of perverse effects of state intervention into the healthcare market, from state laws restricting insurance competition, to severe restrictions on new entrants to the medical labor market, to drug monopolies.
Price discovery requires pricing some people out of the market. Period. There is no "free market" healthcare system that can or ever will deliver required health services to everyone.
Furthermore when the alternative is death or debilitation, the price a "consumer" is willing to pay is effectively everything they possess and can borrow. That is both a massive distortion and non-optimal for the economy as a whole.
There are certainly regulatory inefficiencies and other inefficiencies in healthcare markets, but a truly "free market" in healthcare not morally justifiable.
> Price discovery requires pricing some people out of the market. Period. There is no "free market" healthcare system that can or ever will deliver required health services to everyone.
There is no economic system that can deliver all of the health care to everyone who wants it.
Fundamentally, health care resources are limited: doctors, beds, MRI machines, etc.
Desire for health care is much less limited.
The question is not whether to give everyone what they want, but instead how to imperfectly ration what we have.
We are overspending on the quality of health care we get today. Further there is a lot of fear mongering about socialized medicine.
I've experienced medicine in both the UK and the US. I can tell you, there isn't a difference in quality. Further, when I got a cold and went in, wait time wasn't 6 hours or whatever other BS people claim. Wait time was ~10 minutes. In fact, the time to see a doctor in the US is almost always longer. Why? Because half the time you have to fill out forms and provide proof of insurance and a whole host of other information for them before they will put you on the waiting list.
What did I have to fill out to see a doc in the UK? A card that had my name and current address. Even that, they told me, was optional.
Cheaper medicine for less money is a reality. The only people that lose with socialized medicine are admin and insurance. Everyone else in the nation wins.
I've had different experiences from you. My experience in the UK was wait 90 minutes in a waiting room and when it was finally close to my turn I was told I could only see a nurse and she wasn't allowed to proscribe any medicine so if I wanted to see a doctor I should go down the street to the private doctor. This was in London near Soho.
In Japan the first time I went to a doctor it was for stomach pain. He gave me on ultrasound and declared I had hepatitis. My personel department at my company decided to take me to another doctor. Had to weight 2.5 hours in a room with around 250 other sick people. Was finally told I had food poisoning.
I am not defending the USA system but both the UK system and the Japanese system have issues as well. I've spent the most time in the Japanese system. What I like is it's easy to see a doctor and relatively cheap. Prices are apparently set by the government. Conversely a large percentage of Japanese doctors are quacks and would be unqualified to practice in the USA. It's a common topic of conversation for foreigners here to tell their horror stories of all the crazy experiences they've had with doctors here. Also, top doctors, or rather surgeons are known to require bribes in the $XXXX-$XXXXX range beyond the decided on fees.
I’ve had to wait 3 hours in an ER in America - also have had to drop providers because they only had appointments weeks out.
The decision to go to a doctor is a financial one in the US, sometimes superceding a health one. Our life expectancy is dropping as well. It’s a broken system and adding more of what is broken about it won’t work, if the goal is for society to be healthy.
The UK system isn't amazing, unless you're evidently having an "emergency", you can be waiting for hours (once waited for 4 hours with a broken wrist for example) - that being said, the triage is pretty solid and you'll cycle through intermediate steps in the meantime.
I think the best part is not having the mental burden of potentially going bankrupt afterwards...
There are severe problems with the English NHS, but we need to remember that it costs the tax payer a lot less than the US system.
That's the thing I don't understand: they pay more in tax, and they pay more in insurance, and they don't get universal coverage and have worse outcomes across a range of measures.
Was this with your GP or did you just turn up at the A&E with minor ailments - turning up at the A&E with something you should be seeing a GP with will mean you got the back of the queue.
I have never had a problem getting a appointment to see my GP.
> In Japan the first time I went to a doctor it was for stomach pain. He gave me on ultrasound and declared I had hepatitis.
Ultrasound? That is absurd.
I can't speak for UK/US/Japan but in India situation is quite similar. Opaque pricing along with quacks (or maybe genuine doctors) out to milk as much as they can, especially if they know that you have insurance.
A colleague of mine who had stomach pain was told that he had to get his appendix removed. When he refused the doctor actually threatened him with a write-up to ensure that he doesn't receive any insurance money. After the company got involved he was moved to another hospital, only to be told that he had stomach gas.
When were you in the UK system? I've noticed a lot of variance between people's opinions based on the fact that there's been a sort of sabotage campaign against the NHS in recent years (it's dropped ten places in the worldwide healthcare rankings in the last five years). So people that had experiences with the UK system in the early 2000's generally had a good time, whereas later, it became a lot more mixed.
Assuming you are not an EU citizen, you are don't get free healthcare in the UK anyway. They probably told you to go to the private doctor because if you are non-EU you would have health insurance which would cover this no?
That's not how this works. If you are from outside of EU you are not limited to private doctors and hospitals - you can still go and be seen by any NHS doctor, but you have to disclose the fact that you are not covered by national insurance - they will simply ask you for personal details and send you the bill few weeks later(well, if it's worth if - if you're only seeing a doctor about a cold or a broken wrist they will not even bill you anything because it's not worth the time spent filling out documentation, and pretty much no hospital even has a billing department).
> I've experienced medicine in both the UK and the US. I can tell you, there isn't a difference in quality.
My experience was very different. In January-February this year I had to visit (unfortunately) both the Emergency Room in NYC and the A&E in London. While the quality of the medical equipment in London matches the one in NYC, the understaffing is much more severe. In neither place was my wait time only 10 minutes, but in NYC I had to wait for about 1 hour (including paperwork), while in London for about 6 hours.
I talked with other people in London about my experience that the medical system is severely understaffed, and all agreed. On the plus side, I did not have to pay anything in the UK (they didn't even care that I was not a UK resident). In the US I had to pay north of $1000, despite having insurance.
My Girlfriend managed to stick her finger in a blender in January. We went to a London hospital, got seen by a doctor within 1 hour (she had stitches within 20 minutes of arriving) and she had plastic surgery on her finger that evening. For free.
Different A&E departments have different problems. The NHS is the largest employer in Europe, and it's reductive to say "all London hospitals are understaffed". They are not. Part of the problem is seasonal and even daily shifts in A&E visits, you can't staff for the worst case all the time. And January/Feb is known to be a busy couple of months.
In Boston I recently had to wait in an emergency room for 5 hours with multiple broken bones. This was at one of the best rated hospitals in the country.
I recently moved to a new state and I’m trying to get set up with a new primary care provider. I’ve been trying to get an appointment for six months, but they keep bumping my appointment back. Did I mention that I had to settle for a nurse because none of the doctors in my area are accepting new patients?
This weekend I was feeling incredibly sick and there were ketones in my urine (potentially deadly for me). We got there at 9p.m and weren't seen until 2a.m. They stuck us in the room where they keep patients with potential mental health issues because they were so full so I didn't even have access to a charging outlet. We have good insurance. The US healthcare system is often times just as understaffed. Both can be terrible experiences but one can potentially bankrupt me.
>> I talked with other people in London about my experience that the medical system is severely understaffed, and all agreed.
That is because NHS spending is being slashed viciously. Obviously, if socialised medicine is being dismantled, it can't be expected to work all that well anymore.
Insurance is complicated in the US in no small part because of government intervention.
Starting with the fact that employers pick insurance plans for their employees, eliminating enormous market power: and this happens because the government doesn't tax the money that is spent on insurance plans.
Why did you go to a doctor for a cold? That seems to be a problem. You send someone to school for 10 years and they spend their time talking to patients about a runny nose due to a common cold. And for what? To write a prescription?
For a cold, just wait a week or two. There's nothing medicine can do for you anyway. If it's still there, then it's worth checking. Also, you shouldn't need a sick note unless you are off for more than a week (your legislative framework may vary).
It depends entirely on the employer. Some places will require a doctors note if you miss more than two shifts. So in places like that, people typically go to work sick, and just spread the disease. This includes most fast food restaurants so think about the implications of that.
I wondered the same thing. My mother was a registered nurse who rarely ever took us to a Dr unless we were very sick for several days. For colds she simply treated the symptoms. If we had a fever it meant bed rest and sipping 7-Up to help settle the stomach. The only time she took me was for ear infections and tonsillitis.
That assumes that the desire for health care is unbounded like other consumables.
In reality most healthy individuals want a limited amount of care, sick individuals want the least amount of care required to return them to health - and there are fundamental limits on the amount of care that can be provided to those who are beyond the help of current technology.
As such you would expect a finite level of demand from the economy as a whole if everyone was allowed as much healthcare as they desired. Any attempt at rationing care will both reduce efficiency, and constrain supply - driving up prices. The most market oriented system would leave supply unconstrained and provide universal and automatic coverage allowing more suppliers to enter the market until supply outstrips demand and "prices" naturally fall.
No, the demand for healthcare is basically infinite.
I got a cold yesterday with a crazy bad sore throat, I thought of maybe popping into the doctor. But it turns out to be just a regular cold. My mother would have 100% gone to the doctor. The clinics here in Canada are chock full of kids with the flu and people coming in 'because'. Maybe that's beneficial due to the risk 'it could be something bad'. Or maybe the economics don't make sense i.e. for really mundane things it's better to just stay home and take Tylenol.
But the demand is super high. Once people cross 50, there are always problems. Always something. And it's all expensive.
That’s finite demand as the effort of going to the doctor is non zero. People in good heath are not going to waste their time.
Assuming the average doctor’s visit is 15 minutes and the average person goes to the doctor every month. That’s only 1 GP per 640 people. After that point they might send you to a specialist some fraction of the time, but it’s still finite.
Consider dental insurance is ~15$ a month and most people go to the dentist twice a year. That’s about what GP side of heathcare costs. It’s the care after that point from people with actual issues that gets expensive. Yet, without the vast overhead of insurance you cut the costs of providing actual heath in half. Which more than covers the costs from people that are currently turned away.
PS: And yes billing is ~50% of current US costs when you include Doctor time dealing with paperwork. Remember the entire insurance industry and their profit is pure added cost, but so is the medical billing people inside each provider.
> Maybe that's beneficial due to the risk 'it could be something bad'.
I would assume it's detrimental because it results in doctors' waiting rooms full of people with colds (making it a dangerous place for anyone who is immunosupressed and really needs to see the doctor).
The problem in the US is that you can't just go get your throat swabbed for a strep test in that situation. That could take 5 minutes and cost less than $50, but nope.
Are you saying that the richest country in the world can't accomplish something that already exists in plain view in some of the poorest countries in the world?
There is no country on earth that gives people all the healthcare they might want with no limits and that is not what we should be aiming for. There are many that give people enough healthcare and that is what we should be aiming for.
You really should get the facts on how those systems actually operate.
I'm currently living in an european country that has a national health service that supposedly ticks all the socialist talking points, including free (in theory) access to emergency care, but not only is the service largely inoperational with year-long waiting periods for surgeries, including cancer treatments, but also has a disgruntle workforce who systematically complains they are underpaid and overworked.
The situation is so appalingly bad that the national health service even routes patients to private hospitals and clinics, ending up paying a hefty bill for the services they were supposed to provide in-house but are largely unable to provide.
While I understand your point, I don't know if it could be distilled that succinctly. I have friends who have worked in European countries with universal healthcare that was sub-standard by a U.S. perspective. What I'm curious about is whether this is directly attributable to the healthcare system structure or if it's more causally related to other factors like GDP, access to a trained workforce, or basic infrastructure. Meaning, if we look at two very similar countries that happen to have different healthcare systems would the same effect you outlined still hold?
While I also come from a country like the one you described, there is a very simple fact that cannot be ignored - when my dad got cancer 8 years ago, every single one of his operations and all the drugs(including incredibly expensive Glivec) were 100% free. He was even reimbursed for the cost of travelling to the hospital for his monthly check-up.
If he had the same disease in US, he would die much earlier than he did, I'm 100% certain of it, because quite simply there is no way he could afford the treatment or the premiums that americans are paying for their healthcare. Even when he was sick enough that he couldn't work anymore, he was still 100% covered and didn't have to pay anything for anything ever.
My point is - there are people in our countries who are probably dying because they have to wait months to be seen by someone. True. But there are also people in US who are dying because they cannot afford the treatment they need. I feel like this is far worse than the first situation - after all, we only have a finite number of doctors, a finite amount of hospitals, and limited capacity to add more(for reasons other than financial too). But US is the richest country in the world - and its citizens die because they cannot afford cancer drugs? That's abhorrent.
You have gone from a hypothetical to concluding that people in the US die because they can't afford cancer drugs.
If your dad was over 65, he would be on Medicare. If he was younger than 65 and impoverished (income between 0 - ~150% of poverty level) he would be on Medicaid or another state plan for low income people. If he's above 150% of poverty level he probably has health insurance available at work or thru ACA. In fact is legally obligated to.
It's entirely possible to have health coverage and still be financially ruined by a health emergency due to deductibles and pre-existing condition loopholes.
Medical expenses, unlike credit card debt or student loans, can still be discharged through bankruptcy. For lower income elderly folks, that coupled with low paying job opportunities usually leads to disaster.
> Furthermore when the alternative is death or debilitation, the price a "consumer" is willing to pay is effectively everything they possess and can borrow.
This is also true with food. What keeps the price down is competition, not price controls.
so when I get into a car accident and am bleeding internally, I can march down the street to the next hospital if I think the bill at the one I'm at is too high?
No; but suppose we agree that emergency response services (fire, medical, police) should be state-run. The goal of such state-run ER is to get you as quickly as possible to a hospital, where care can be provided. The state can then shop around for the cheapest/best private provider for each catchment area. One could also make a case that the state should pay for this emergency care out of tax money - unless the state can show that you were the one responsible (e.g. if you end up in a hospital because of excessive drinking on a night out - taxpayers should not have to pay for you in this case).
But such true emergency response seems like actually a very minor part of all medical care. It would be better for people to have private emergency arrangements through their insurance - but, of course, this is not always viable (if you are bleeding out in a car accident, there is no time to figure out which hospital you have a deal with), so that is one area where the state should probably be involved.
Does it have an end goal of maximizing profits, though? Couldn't the goal of price discovery be to find the point where supply = demand, without necessarily maximizing profit?
Granted, this ignores the human trait to increase consumption when removed from directly paying all associated costs (e.g., my behavior at Golden Corral)
Doesn't that imply they compound profits by either 1) raising prices and thus reducing demand for their product in the presence of non-profit maximizing suppliers or 2) creating efficiencies to increase profit margin at an equal-or-lower price?
In situation one wouldn't the advantage go to the non-profit motivated supplier and in situation 2) doesn't it ultimately benefit the customer with lower prices?
I think the point is if one company is making outrageous profits it’s trivial for a competitor to undercut them. The food industry for example rarely makes more than 2% in profit because it is so competitive.
I would agree, but only with industries with a low barrier of entry of commodity businesses. There are also other moats that prevent trivial competition. Examples may be intellectual property, branding, switching costs etc.
I see your point if the term profit is defined in a general sense, but with the exception of "corporations as people" caveat there's plenty of everyday examples where people are trying to maximize outcomes other than capital (sometimes at the expense of capital). I'm not sure that makes it any less of a free market
It does. There's no free market for soup kitchens for the homeless, for example.
There exist entities who are willing to provide soup kitchen services below operating costs in perpetuity (i.e. charitably, for free). The price for services is kept artificially low ($0) by constant infusions of capital from outside the market (charitable donations), which prevents for-profit vendors who don't receive constant cash infusions from being able to compete on a level playing field. The resulting market is thereby warped by the distorting influence from non-market forces, preventing it from operating efficiently. It's not "free", in the technical sense.
This isn't necessarily a bad thing, to be clear. The charitable funding system may well provide better aggregate social outcomes than a free market would for any number of reasons, not the least of which being that one of the freedoms that "free market" implies is the freedom for vendors to decide that some of their potential customers are more trouble than they're worth to serve.
You illustrate the point well and maybe I'm just not well versed enough in the topic. You imply that a charity warps the free market by undercutting profit-motivated competitors but in the last statement you give the vendors the freedom of choice in regards to their customers. Is there any reason why this same freedom of choice can't be extended to people who choose a specific social outcome at the cost of less (or nil) profit? For example, are B-Corps fundamentally less "free market"? Or does the very nature of free market imply a profit maximizing function? As an example that comes to mind, I'm curious how not-for-profit and for-profit hospitals interact in a "free market" of healthcare in the United States.
> Furthermore when the alternative is death or debilitation, the price a "consumer" is willing to pay is effectively everything they possess and can borrow
Someone is morbidly obese. They will die and are already debilitated. The cost of having their life back is eating less. Many are not willing to pay that price.
No, a well working competitive market reaches a price where marginal revenue equals marginal cost. Unless you are using an unorthodox version of microeconomics.
> There are certainly regulatory inefficiencies and other inefficiencies in healthcare markets, but a truly "free market" in healthcare not morally justifiable
Socialized healthcare has its own "immoral" trade-offs. We essentially reduce per capita quality in favor of all-inclusive coverage. Proponents of free-market healthcare would argue that the inefficient allocation of resources inherent to socialization is immoral. Libertarians would argue that forcing money from one person to give to another for medical care is immoral. It's not really a question of morality, more of preferred philosophy and practicality. Framing it around morality makes the other side seem abhorrent and the situation difficult to find common ground.
> Socialized healthcare has its own "immoral" trade-offs. We essentially reduce per capita quality in favor of all-inclusive coverage
That's a false dichotomy; there are many mixed systems where the government provides a baseline level of care with private insurance providing additional services or benefits (eg: government covers a shared hospital room, private insurance covers a private room).
>Libertarians would argue that forcing money from one person to give to another for medical care is immoral
True libertarians also argue that all taxation is theft (if they're purists anyway), making road construction immoral.
> Framing it around morality makes the other side seem abhorrent and the situation difficult to find common ground.
A "free market" in healthcare requires us to condemn people to death or debilitating injury when they cannot afford care. Unlike nearly every other area, this one literally involves life and death so I believe it must meet a different standard than other activity (economic or otherwise).
> True libertarians also argue that all taxation is theft (if they're purists anyway), making road construction immoral.
No, it doesn't make road construction immoral in the eyes of libertarians. It makes taking money from other people, by force, in order to build a road, immoral. People are totally free to build roads privately and pay for it themselves, and even band together to build these roads.
(Part of where the standard libertarian argument falls apart, in my eyes, is that government in many ways really is just a scaled up version of "people banding together to build a road". There are there are legitimate moral/philosophical questions around opt-in vs. opt-out though).
> Part of where the standard libertarian argument falls apart, in my eyes, is that government in many ways really is just a scaled up version of "people banding together to build a road".
There is a significant qualitative difference in that "people banding together to build a road" is an entirely voluntary activity, whereas government is nothing of the kind. It's not merely a matter of "opt-in vs. opt-out". Even in an opt-out system one can choose not to participate without penalty, but if you inform a government that you're choosing to "opt out" they won't just leave you alone to live as you please. They draw their arbitrary lines on a map and consider everything within those lines to fall under their control. Even if you move halfway around the world and renounce your citizenship, and in doing so cut off all ties to everyone and everything you once knew, you may find that they still claim a share of your income to pay for that road you'll never be able to use.
The "scaled-up" version of "people banding together to build a road" is a co-op or corporation. Such an organization does not have the power to tax or to impose regulations on anyone who doesn't explicitly and voluntarily agree to them.
> True libertarians also argue that all taxation is theft (if
> they're purists anyway), making road construction immoral.
Why would you call those people "true" libertarians? There are a lot of people who consider themselves libertarians of various sorts who strongly disagree with this. Some consider property to be theft.
There are many kinds of libertarianism, and the American-style extreme capitalist libertarianism is not the only one, and probably one of the most irrational forms of libertarianism.
Personally, I feel providing essential care to everybody equally does the most to free people from oppression and extortion by those who wield power over them at a time when they're vulnerable.
Exactly. It's the same reason we don't have free market police and fire services. You simply don't get to "shop around" for emergency services, which includes privatized ambulance services (which are outrageously expensive, on the order of $12,000 for the ride I took when I had to take one, and it was a relatively benign one... thank god I had insurance). EMS is covered, but that's the Fire Department. After that, it's all privatized.
If it's cosmetic, then I could see the argument. But when it comes to emergency services, and for ambulances especially, the "free market" argument just doesn't hold water.
The history of private firefighting is a particularly dirty one.
In the past, fire companies would show up and demand payment before putting out fires. If a payment couldn't be made, the company might negotiate the purchase of the burning property at a steep discount.
Later, insurance companies hired brigades to only put out fires on insured properties. Fire companies might have fought or sabotaged one another in order to win the right to put out a fire and get paid for it.
While it isn't perfect, and it's often underfunded, I definitely prefer the system we have now.
Not everywhere, though. In Denmark, private operators have been handling emergency services since 1926; currently one company (Falck) is handling 65 percent of municipal fire brigades and 85 percent of ambulance services. No particular nastiness has been reported afaik.
Right, but that's not paid for by the end customer (at the point of use), is it? There could be single payer with private doctors they'll just get paid with public money, which is entirely different to Joe paying his doctor.
The US has lots services that are provided by regulated monopolies. My garbage company, power company are all regulated monopolies. A key thing is you're required to have garbage and power service but the rates are negotiated by a public utilities commission or the city or county.
However Healthcare in the US isn't a regulated monopoly like that.
My point was just we do have regulated monopolies in the US. But healthcare in the US isn't a fully regulated monopoly.
I'll argue whatever PG&E problems are they don't rise at all to the level of healthcare. And their problems are due to poor regulation and the US's current terrible management culture.
I think this is because the culture is quite different in DK compared to the US. There is an expectation of how it will work which is very different by everyone involved.
No, it's because ambulance service in Denmark is a public contract. Private citizen don't pay out of pocket.
Essentially, the state (or region) contracts a company to deliver ambulance services. The contracts usually last a few years and are limited to a region.
Furthermore, the company that wins the contract (usually lowest bidder) is held accountable is too many responses are too slow, etc.. usually with hefty fines.
I guess you can call it privatization, but it's more of a regulated monopoly. Ultimately, these things outsources uncertainty from the state to the private sector. I'm not convinced it's always a good idea, since companies can just factor the cost of fines into the contract... Granted if there is competition, it can drive the prices down a LOT.
And public contract it is in many other places, like where I live (Finland). Local government pays ambulances, I pay a sum to the local government out of my pocket after I have used ambulance.
In the past, fire companies would show up and demand payment before putting out fires. If a payment couldn't be made, the company might negotiate the purchase of the burning property at a steep discount.
Usually credited to Marcus Licinius Crassus, who had a fire brigade for just that purpose. Contemporary of Julius Caesar.
I have a vintage fire plaque next to my front door. They were commonly issued long ago to show that insurance has been purchased. No plaque, no service.
> Later, insurance companies hired brigades to only put out fires on insured properties.
In some parts of the world, insured properties were marked with metal plaques (generically termed "Fire Insurance Marks" [1]) bearing the insurer's symbol/logo. This enabled the insurer's firefighting service to verify that they should protect the building. I've occasionally seen them on old buildings here in the UK. One I remember was a stylised representation of the sun, denoting The Sun Fire Office - which was founded in the 1700s and still exists as RSA Group plc.
Later, insurance companies hired brigades to only put out fires on insured properties. Fire companies might have fought or sabotaged one another in order to win the right to put out a fire and get paid for it.
There are analogies (with smaller consequences) in private tow truck operation.
I'm pretty sure not. The term "fire sale" refers to selling merchandise that survived a fire and therefore would have associated damage.
However the policy of negotiating for property at bargain basement prices while there was a fire next door was very notably one of the ways that Marcus Licinius Crassus (a political ally of Julius Caesar) enriched his fortune.
With our level of inequality, this is coming back. In the last Southern California wildfire, there were reports again of private firefighting groups operating in the Malibu area.
These private firefighters are generally contracted to government agencies. This is the same thing the US government or CALFIRE will do during any Type 1 incident.
The same as a concert promoter hiring off-duty cops.
Ah, I understand that happens, but that's not what I was referring to. I was referring to private homeowners and insurance companies hiring firefighters.
Companies like Rural/Metro, traditionally ambulance/EMS companies, have expanded into private fire, in those places (one notable city is Grants Pass, OR).
This is a wildly different situation than what the GP was talking about. If you have the means, why wouldn't you hire a private crew? The public crews are there to get the best outcome at a macro level, not to protect your house in particular.
It's not clear to me it is different. You still have a divergence of motivational coordination between public fire teams and private ones. For one a private fire team can force public ones to stay committed to areas by not heeding evacuation orders...
Why is this dirty? If you don't pay for fire protection, not even through taxes, why does anyone owe you incredibly hard & extremely dangerous labor saving your house? Firefighting is not a safe profession.
It's not the payment that was specifically dirty, it's that privatized firefighting was a dirty job historically in America. Like competing companies brawling in the street on the way to a fire, dirty.
" the company might negotiate the purchase of the burning property at a steep discount."
This creates the perverse incentive to demand an outrageous price so they can get an property for cheap. Next step would be setting fires to buy even more property.
Without their offer, the market value of the property is zero. Who is going to buy a house that has no fire insurance and is currently on fire? Is a steeply discounted price really outrageous? They might perish in the fire, they might fail to save it. Firefighting back then was no sure thing.
Now, if two crews showed up and bid against each other, things start to get interesting.
If two crews have to show up for a fire... That means higher prices because most of the time there is no fire, so they just sit around waiting -- more people higher cost.
It also means it might be that nobody shows up, because it's a holiday, so nobody was on duty.
Public services are often incentivized to create more work to protect their jobs. Famous examples include whatever department was enforcing prohihbition in the 20s to find other things to prohibit when alcohol prohibition was repealed. In Japan it's common to see unneeded road work because if the entire budget it not spent it will be reduced.
Sabotage and physical fights broke out between fire companies while fires burned. That's a pretty gritty situation.
Allowing fire sales gives way to perverse incentives, like the profitability of arson and predatory pricing of fire fighting fees such that certain portion of victims will always have to sell their property at a discount.
In theory, all of this also applies to a public "firefighting department", no? They too could do a really, really poor job. If this is the culture in a society, where people want to screw each other over, you are likely to get this poor outcome regardless.
But suppose that you have an honorable firefighting department run by an honorable man. Why could he not have set up a private firefighting company instead, doing pro bono work when required? Given the honorable behavior of his company, why would consumers not want to prefer him for insurance than shady competition, which may be cheaper but is also more likely to screw you over when you most need them?
Government-run agencies can be good or bad; private companies can be good or bad. There is no silver bullet and much depends on the prevailing culture. But government can use the threat of force to compel you to pay for their services. If a private company attempts the same, we would call it an organized crime group.
> If it's cosmetic, then I could see the argument.
Then there's another problem: who defines what is considered "cosmetic"? Most insurance companies currently don't cover e.g. facial feminization surgeries for transgender women, even though they're considered medically necessary by WPATH, a document drafted largely by insurance companies [0].
I said I could see the argument, not necessarily agree with it. I mean, in this day and age insurance companies also consider a severe cleft palate a cosmetic surgery and not a necessity. I certainly would not leave it up to them. I think it should be left up to the consult doctor, to be honest. If you don't agree, consult another =/
So prices are excessive because too many people don't pay their bills, leading more people to be unable to pay their bills, leading to even higher prices.
So my 15 minutes $600 allergy appointment that insurance refused to cover (after covering the same damn appointments for 12 years) is that high because of others, or so I keep hearing...
But yeah, I assume it's a combination of:
* Most people pay through their insurance, so they don't have to pay the sticker price or anything resembling it
* Some people going on payment plans and getting stuck in debt basically forever
* Some people bargaining their bill down, paying pennies on the dollar
* Some people going into collection, paying pennies on the dollar
Of course, it's absurd that all 3 out of 4 paths require you to take extra, often really painful steps (collection + bankruptcy, maintaining insurance, or long drawn-out negotiation) just to pay a reasonable price for something that is 100% non-optional and most countries provide for much-closer-to-free. But that's kinda what happens when the system is broken
There is so much good that price transparency would do. Most treatments are not emergency and you can absolutely shop around even if it's not cosmetic. Ever hear of medical tourism? It's not a perfectly 'free market', but it could benefit so much from better information.
Following the current government's cutbacks to the state-run police, residents in one part of London (which is incidentally the "one of the safest ... seats in the United Kingdom"[0] for the current government) have funded their own private police force[1]. This is apparently working out well for them. The issue is that it furthers the division between the rich and the poor, with proper protection from crime becoming available only to the wealthy.
Those aren't police forces. From my reading of the articles, they do not have the power to arrest people, serve search warrants, evict people, etc. They do do detective work and security work.
> A free market police system cannot work, because the police use force against people, which is not allowed by the free market.
The "free market" (in a libertarian sense) does not permit the initiation of force against people who have not resorted to force themselves. If that is a significant restriction on your police department's activities then there is something seriously wrong with your police department.
> Worse, the police aren't going to arrest people who pay them.
If they aren't willing to arrest anyone who pays them then no one will bother to pay them. Resolving disputes between two paying customers is part of their job description, and they won't retain customers if they're seen as biased or corrupt.
Arresting someone suspected of a crime is not responding to initiation of force, because the suspect hasn't been convicted yet.
There are private police forces, we call them the "mafia", and people pay them for "protection". Sure, they're corrupt, but with no government funded police, whatcha going to do about it?
> Arresting someone suspected of a crime is not responding to initiation of force, because the suspect hasn't been convicted yet.
If the suspect is eventually convicted (of something at least as serious as kidnapping) then that conviction retroactively justifies the arrest.
If the suspect is never convicted then arresting them is little better than kidnapping. If the police at least had a reasonable belief that the person they arrested would be convicted then it falls under the heading of accidental harm rather than negligence or malicious intent, which shields them from retribution, but that doesn't avoid the need to pay restitution to make their victim whole.
In short: Be sure you're arresting the right person, and don't do anything to them in the process which you'd find difficult to set right.
Arresting someone is no joke and cannot be done using free market principles.
Enforcing laws is the point of government, and a free market requires enforcement of laws. This is why countries with a non-functioning government are an anathema to business, not a paradise.
> privatized ambulance services (which are outrageously expensive, on the order of $12,000 for the ride
What state? In Washington (and many, though definitely not all), ambulance prices are regulated, for this reason. When I worked private ambulance a couple of years ago it was $680 + $8/mi.
Seattle, but I guess I had some perks. I didn't itemize it. That was for everything. They did not take me to the closest hospital, either, for some reason.
Although most humans are perfectly ambulatory, there are innumerable reasons why they don't get to "choose where to live". Income levels, employment availability, schooling, racial pressure, and many more factors come in to play. Not everyone can physically fit into the best areas. The best areas for emergency services don't necessarily align with the best education (although very high income levels tends to align with both). This comment essentially amounts to "Well if you don't like being poor, then just obtain more money". While everyone cannot live in the best places, nearly everyone will need emergency services at some point in their lives. Also, OP didn't suggest getting rid of private care entirely. A public option does not preclude a private system. If the private system provides value, it will likely survive.
The biggest complaint of public systems is wait times for services. If the rich can jump ahead and get treatment ahead of the poor then congratulations you've built a system that enables the rich to pay for life saving operation, while the poor do not. Right wing parties then spend their time in power weakening the public system so those wait times increase or quality of service lessons.
Another way of looking at it is we don't have private firehalls. I'd argue healthcare is the same.
Interestingly we are moving towards having private security forces, enabling some to be more safe than others. I don't agree with that either. So, maybe it's a philosophical difference, I feel strongly that for basic rights (e.g. health, safety) we should all be treated equal, and money should not grant me special treatment.
> If the private system provides value, it will likely survive.
And if it doesn't survive, good! Industries don't have an inherent right to keep existing if they don't fill some useful function. Refusing to implement an otherwise desirable social program because it might cause an existing industry to become obsolete is far and away the most anti-capitalist argument I see self avowed capitalists make.
You haven't rendered private health care "obsolete", you've just forced people to join your public system. Obviously people aren't going to pay for two health providers (unless the public system is completely inadequate). That does not imply that the private service is uncompetitive. There can be no competition when one service must find willing customers while the other takes its funding by force.
This is the same issue with toll roads vs. public roads. Imagine there are two similar roads leading from A to B, one a toll road and the other public. The toll road charges drivers $1 per 100 miles. The public road is free to use but costs every driver $5 per 100 miles in taxes. Which one do you think drivers will take? The more expensive public road, of course—because they're already paying for it, whereas the toll road would be an additional expense.
True, but that's subtly different than the point I'm trying to make.
Imagine your hypothetical were reversed. Imagine we already had a network toll roads priced at an average of $5/100 miles, and that we had a plan to build and maintain public roads at an expected cost of $1/100 miles. There might be plenty of good reasons not to prefer the more efficient public plan, but the fact that it would put toll road vendors out of business isn't one of them.
Capitalists don't mindlessly prefer private things just because they're private. We like them because they tend to self-optimize for efficiency more effectively than a centrally managed system can. Usually. There are a whole thread's worth of reasons to believe health care is one of the exceptions, both in theory and in practice. If that's the case, then refusing to implement a superior public system solely because it would decimate the inferior private one is just another flavor of the same anticompetitive protectionist bullshit that makes tarrifs and professional licensing and restrictive zoning and a dozen other types of cronyism distasteful.
> There might be plenty of good reasons not to prefer the more efficient public plan, but the fact that it would put toll road vendors out of business isn't one of them.
I have no particular sympathy for any private provider that can't compete with other private providers in the market. However, from my point of view private and public providers aren't in the same market, or even providing the same product: one is simply selling access to roads, or health care, while the other is giving these things away bundled with the dubious "service" of compelling other people to pay the bill. To me that bundled "service" is of immense negative value, and the existence of the public system is driving the providers of the unalloyed product I actually do want out of the market. So, from my point of view, the fact that the public plan would put the toll road vendors out of business and thus leave me with no decent travel options that don't involve externalizing the cost onto others is actually a good reason to oppose the public plan. (There are others: While I don't want to participate in this externalization process as an unwilling beneficiary on moral grounds, I'd also prefer not to become one of its victims.)
Of course, if there exists a way to build and maintain a road at a cost of $1 per 100 miles, there is no particular reason why that cost couldn't be payed through tolls instead of taxes, thus giving us the best of both worlds. There are basically only two ways which public services can manage to cut costs compared to a private provider. One is by externalizing the cost of the service onto non-users, and the other is by being exempt from regulations which private providers would be forced to follow (or, equivalently, having the regulations tailored to suit the public service by sympathetic legislators).
> Capitalists don't mindlessly prefer private things just because they're private.
Whereas libertarians such as myself do prefer private things simply because they're private, which is to say: because they don't involve the use of force. Which is not to say that there aren't practical reasons to prefer private systems as well—just that, to me, any system which involves force is automatically more costly than any voluntary system, which makes these other reasons more-or-less irrelevant.
True to an extent, but in any city (100,000 or more people) there will be two hospitals and so the poor can choose which of the two to use. Note that by poor choosing only a small number need to have the practical ability (which is to say the almost middle class) to choose since a hospital will want to attract them and that ups service for everyone even thoose who couldn't reasonably get to the other hospital.
You know the hospitals in this scenario wouldn't be next door to each other, right? The extra 30 minutes of driving time it takes for me to get to my second-closest hospital could easily mean life or death.
For the person 15 minutes from either hospital there is a choice though. Trying to attract those middle people results in better services for those who are clearly closer to one hospital.
In addition to what other people have said about the impracticality of assuming choice, said hospitals will often not offer the same set of services, or will specialize in certain aspects of them.
You rarely have this choice in practice. Plus, as the article points out, even if you chose an in-network hospital you may well be seen by an out-of-network doctor.
In a free market the incentives are different though. in-network only is a thing because hospitals don't have any incentive to ensure everyone is in network.
>> You simply don't get to "shop around" for emergency services
> You do actually, by where you choose to live
That's wrong on so many different levels:
1) The emergency service provider is unlikely to tell you how much anything costs in reality ahead of time.
2) Not all emergency services providers offer the best price for all services, or are even equipped offer all services.
3) Many medical emergencies are completely unexpected, you have no idea what kinds of services you'll actually need in an emergency.
4) You're not really talking about "where you choose to live," but rather "where you choose to be at all times." Do you really have a choice of ER if you have to stay within a couple miles of it at all times to make sure you'd always be taken there in an emergency?
I don't think there are many places outside repressive states where private healthcare is actually banned? Even the UK's extremely centralized NHS runs alongside a private system. It actually has the effect of making the private system cheaper since they don't have to cover everything or everyone.
That's a stretch. There are still a lot of private clinics operating in Canada for various grey-area medical needs. Also, Canadian (really, provincial) healthcare doesn't typically cover dental, and there's a massive grey area in rehab and injury recovery where private clinics abound.
Certainly it is true, I agree, that emergency hospitals and ambulances are public-option only.
Based on the success of private MRI clinics, I would say the demand is quite high for selective procedures. Either procedures that are relatively cheap but have very long wait times or procedures where patients are willing to pony up for expertise (joint surgery).
"Move to a better market" seems like an argument that some local marketplaces have failed. The whole value proposition of the free market is that it improves the available services and prices through competition. If I have to move somewhere else to find a market where this is true then the local market is clearly failing and the free market idea doesn't work.
Said another way: Should I then also move when I want to find a better price on milk?
"Move to a better market" also fails with regards to the fact that you may need the services when not at home. If you were working in sales would you refuse to do an onsite meeting with a client because their office is near a terrible hospital?
Did they leave Hawaii only because of the price of milk or because staple goods in general were more expensive than other places? In this case the market is working but it is a market where cities compete on cost of living, not milk. In that case moving makes sense.
> I think there's merit to investigating public health care. That line stops for me in eliminating private care.
Has anyone proposed that? If not, I'm not sure why you mentioned it.
Anyway, I suppose I can see the benefit to private doctors, but if private emergency response services for individuals are popular, then something is fucked, as your link demonstrates. Not saying they should be banned, but they shouldn't have to exist in a properly-run society.
What serious single payer proposals have been put forward that would eliminate private-pay, private insurance, or private care?
I've never seen one.
In fact, almost all "single payer" health systems that exist in other countries have private care and private insurance options. For example, such options are available in both the UK with the NHS and in Canada.
I've never once spoken with an advocate of single payer who wants to eliminate private pay, private insurance, or private care.
I am also an advocate of single payer, and I wouldn't advocate eliminating any of those things.
It most definitely means banning private insurance (not private care). Thats why its "single". IT has to, because otherwise it would have to compete on the market as any other plan, and it would fail because all private insurance would dump the expensive patients on to medicare, which will need to either increase prices or increase taxes to survive.
Plus the whole point is to eliminate dealing with the adminsitrative burden of claims and billing. IF you just add another insurance, you just make it worse.
No, the single payer portion doesn't have to compete with other plans. The other plans supplement the single payer insurance. E.g. single payer will cover everything up to a certain amount, and then you can buy a private plan to bring that amount higher, or maybe cover non-essential extras.
Ofc you can invent an infinite amount of models, and Sanders has not specified which one clearly yet afaik.
In the case that Medicare is expanded and is optional, medicare will have the following fair challenges: it has to compete with other private insurances, which means is has to pay as much, and any administrative cost dissipates, in fact it gets worse, as providers still have to do multiple billing.
If it has to charge ,it will also have to turn away patients. It it doesnt charge, everyone will have medicare, and private insurance will not provide services that medicare gives for free or without restriction.
Up to this point, "single payer" has not provided a single cost reduction means.
Didn't know this existed, thanks for sharing. (I got my other impression by Sander's fb which I follow).
If I understood this text correctly, this will be:
An optional insurance plan (SEC. 105)
An insurance that gets tax benefits (SEC. 701)
An insurance that has incredibly perverse utilization incentives (SEC. 202)
I would be quite on board on this plan if it weren't funded with special taxation, and it gave itself no promise of benefit for being the state, not because I think its a good one, but because it will confirm its a terrible one.
"Single payer" means the state pays through the tax system. It doesn't mean banning private insurance, which coexists happily with the NHS. Whoever told you otherwise has been misleading you.
This is quite evidently rubbish, as demonstrated by the fact that I live in the UK, receive most of my healthcare for free, on the NHS and also have private medical insurance (provided by my employer).
The problems the UK has and the US has are completely different. Starting with the fact that the model of providing both a public and a private insurance system in the US will not save a single buck.
Saying that Sanders is advocating the elimination of private health insurance because he favors Medicare for all is just as inaccurate a saying that anyone who advocates for improving public transit is trying to eliminate all privately owned vehicles.
I'm sure there are plenty of things to dislike about Sanders or anyone else whose political leanings tend toward things like publicly-funded healthcare coverage, it should be possible to come up with a few of them without blatant misrepresentation
Both Medicare for all and Medicare buy in plans wouldn't eliminate private health insurance.
Private health insurance would still exist under both plans as supplemental coverage that people could buy that would cover things that were not covered by medicare.
The markets would be potentially reduced (drastically with medicare for all, moderately with a generally available medicare buy-in), but it's totally false to say they would be eliminated under those plans.
Are they on felony probation? I have moved a few times with little money for better opprotunities. It seems like most people are just psychologically conditioned to die near where they were born. Most people just think the hardship is worth it, which is very much a choice. It is literally cheaper to move to most of the USA than live another month in places like california or nyc.
This ignores a huge array of practical reasons why people stay where they are.
Family networks are probably the number one reason. Child/elder care, food/housing/etc. sharing and a lot more are all major factors that by definition do not show up in economic reports.
And that's before people's "psychological conditioning" (which some people refer to as "being part of a family") is considered.
I, too, have moved around a lot - across the US three times, overseas and back once, with smaller cross-state moves in between. And it has worked out for me. I am also not married, have no kids, am not very close to my family, have a high degree of risk tolerance and high attraction to novelty, and seem to need a smaller community of folks in my life than many others.
I'm also well aware that I am an abnormally-unattached person. Most people have significantly more difficulty uprooting and moving somewhere else. Writing that off as conditioning that interferes with economic concerns not only fails to recognize very real economic aspects that don't show up a bank account, but also fails to recognize that humans value things other than money.
We do not have a free market. Most people get their health insurance from their employer - you cannot reasonably get insurance elsewhere (the same plan I have now for $100/month would cost over $1000/month, but I can't take that $1000/month to anyone else if I don't like my insurance so I accept it). This keeps me from taking a long leave of absence to live off my savings - until I quality for retirement (medicare).
In a true free market you would have more choices: most emergencies are close to home so you are likely to know which hospital is a good deal.
Of course there are still the emergency while on vacation, and the sudden collapse where a bystander brings you somewhere which are harder to handle. Though if there really was a free market there is incentive to handle those well - if only because the system is designed for the majority of cases where they have to handle it well or you would have gone elsewhere.
> We do not have a free market. Most people get their health insurance from their employer - you cannot reasonably get insurance elsewhere
What you are describing are in fact the freest parts of the health insurance market.
Employers, quite rationally and of their own free will, choose to offer health insurance as a benefit because it attracts and retains talent better than other similarly priced incentives. The fact that you're hesitant to take a leave reveals that it's working.
Insurance companies, quite rationally and of their own free will, choose to offer steep discounts to purchasers who buy for a large group of people instead of just one or two. It reduces their marketing costs and gets them a better balance between sick and healthy clients.
You, quite rationally and of your own free will, choose to both accept your employer's offer of discounted insurance and to remain at your position longer than you would otherwise prefer to maintain that insurance coverage. In fact, the only thing you foresee changing the status quo and allowing you to retire at all is when you become entitled to benefits from the state in the form of Medicare.
Nothing in the phrase "free market" implies the resulting equilibrium won't conspire to limit an individual consumer's choices.
> Employers, quite rationally and of their own free will, choose to offer health insurance as a benefit because it attracts and retains talent better than other similarly priced incentives. The fact that you're hesitant to take a leave reveals that it's working.
This is false. Offering insurance as compensation started during WWII when wages were frozen by the government. Employers found other ways of attracting workers.
There is also the fact that employer-provided insurance is almost entirely untaxed. A dollar in direct employer insurance is essentially a dollar directly to healthcare spending. If it goes through to the employee, that's reduced to at most $0.70 due to payroll taxes, and often much lower. This provides and incentive for both employers and employees to prefer employer-provided insurance.
Compared to these, the effects you described are negligible.
> Offering insurance as compensation started during WWII when wages were frozen by the government.
Absolutely true, and those regulations haven't been in effect for the better part of a century now.
If you want to argue that long-discontinued government programs can entrench systems that continue to produce market distortions today then I'm happy to agree with you, but that's the exact stated rationale for the broad suite of civil rights regulations that in my experience most libertarians oppose on economic freedom grounds. I don't think you get to have it both ways.
> There is also the fact that employer-provided insurance is almost entirely untaxed.
Again, true. But I think you're drastically underestimating how beneficial it is to an insurer to cover groups of mostly healthy people (i.e. a company's entire labor force) instead of groups of mostly sick people (i.e. those most motivated to acquire private health insurance).
In order for the market for healthcare to be truly free, in the sense you're describing, medical professionals would need to be willing to consistently refuse service to people who can't pay, which is frequently in violation of their professional ethics. Since that (entirely private and voluntary) market distortion isn't going away any time soon, insurers who can find other mechanisms to incentivize relatively healthy people to contribute to the risk pool can provide the same coverage at a lower cost per person.
That means that, tax incentive or no, insuring a broad cross section of mostly healthy people as a group is always going to be cheaper than insuring them individually. And the more healthy people can be incentivized to sign up, the cheaper it becomes for all participants, which gives whoever is making decisions on behalf of the group an incentive to encourage as much of their potential pool to participate as they can. The taxes reinforce this system, but it would still be self-perpetuating without them.
"Compared to these, the effects you described are negligible" is also a positive claim, and I did at least as much work sketching out why I believe my claim as you did sketching out why you believe yours.
I don't dispute that the current status quo emerged as a direct result of government intervention. Again, I agree with you that it can be traced back to WWII era wage controls.
My claim is that, once established, the resulting equilibrium is economically stable. Your claim, as I understand it, is that it's not.
Given that the price controls that we agree created the current status quo were replaced by significantly less coercive tax incentives decades ago and to the best of my knowledge the industry hasn't attempted to realign away from employer-provided insurance since then, I don't see a reason to privilege your hypothesis over mine.
Employers offering health insurance as compensation is a legacy of wage controls from WWII. Employers were prohibited from paying market-level wages so they offered health insurance. It is entirely a result of non-free-market government controls.
"Employers, quite rationally and of their own free will, choose to offer health insurance as a benefit"
Sorry, it's because of tax breaks, not pure rational free market. All the rest of what you describe are unintended consequences of that non-free-market tax break that seems like such a good idea on the surface.
Is this the magic phrase that means "free market" to you? Because the word "free" is in it?
We could say that the USSR, quite rationally and of its own free will, sent millions to the gulags and forced labor camps to create widgets. Cute, right? Hey, they did it quite rationally (after all, the labor is way cheaper when you're using prison camps) and of their own free will, therefore it's the free market!
We can't say the prisoners chose to enter the gulags of their own free will, though. Since freedom of contract requires all parties to enter into the agreement consentually, that means that the market for gulag laborers is not free.
The US governent does create incentives which change the optimal behavior of rational actors in the health insurance market, but those actors still have very broad latitude to respond to those incentives as they see fit. That's not perfect economic freedom, but it's a lot closer to it than the systems most other countries use. It also gets noticeably worse results on a broad variety of metrics than the systems most other countries use. Make of that what you will.
And the reason that healthcare costs $1,000/month, is because this system has caused prices to spiral completely out of control, beyond the level of lunacy. Due to multiple agents in the market behaving of their own free will.
Every other developed country manages to provide equivalent care for a fraction of the price. So much for the free market optimizing for better outcomes, eh?
It's about the same price, except you're totally covered and it includes your pension. Oh and you don't even see the money, it's paid by your employer directly.
You are missing one critical point though: If I through my own free will decide that I want a different plan I need to come up with that $1000 difference that my employer is kicking in for me. If I could get that $1000 back to spend on my own I'd have the ability to choose a $1300 plan instead of the $1200 plan (for $1100 because of the factors you sight), that extra $200 out of pocket is much more affordable than the extra $1200 I have to come up with now. Or maybe I don't want all the perks of my work plan would want a $1000 plan that doesn't cover something in the work plan.
Gee, that sure does sound like a private dispute between you and your employer to me. If you want to opt out of your company's health care plan then you're more than welcome to go attempt to negotiate with your manager about raising your salary by the amount of their health care contribution. Best of luck to you.
Group plans distort the risk pool and are disallowed in countries like Switzerland that require health insurance. The major problem with the ACA is that they didn’t eliminate employer group plans, leading to an apartheid like situation where those higher income people having a discounted rate because the group pool they are in is much safer than the pool poorer people on the individual market are put into.
What is worse is that poorer people in the individual market can’t even get a tax break for buying health insurance (not until it becomes 10 percent of their income and they decide to itemize). In contrast, employers buy health insurance for their employees tax free. This literally screws poor people in service jobs by making them actually pay much more for health insurance (even including what the employer would pay).
$1000/month is probably a heck of a plan or in a really expensive market if it's for a single person, and it's probably still decent for family coverage. If it was through the ACA Exchange it's probably also a Gold plan that when you look at maximum out of pocket costs simply loads up the premium rather than the OOP payments.
In California the cheapest plan is about $450/month from the Obamacare marketplace, so I'm not sure $1000/month is going to be that outstanding. And as I understand it, $450/month is about the minimum a plan can cost, since Obamacare outlawed the old high-deductible catastrophic insurance.
Also, I doubt that the average family has $12,0000 of medical bills a year, and would be better off paying out of pocket except for that fact that bills can be randomly expensive.
Obvious typo aside ($12K not $120K), this is entirely the point of insurance. If the average person would save money by buying insurance, then the insurance company would be losing money. In general, if you can afford to pay for the worst case scenario, you are always better off without insurance (BTW, this includes "extended warrantee plans" hint, hint). Insurance is for things where your can't afford the worst case scenario.
Yep. You get a choice to be gouged on premiums or essentially gamble, hoping that life doesn't reset your savings to $0 (or lower) by getting in a car accident or something.
It's actually not quite as bad as that. My personal preference is for things with copays instead of coinsurance, but beyond that if you look at the maximum out of pocket for most of the plans there's not that much difference between Bronze, Silver and Gold. The big difference between a lot of them is whether it's frontloaded (high premium, lower deductible, higher percentage coverage, lower copay) or backloaded (lower premium, lower percentage coverage, higher deductible, higher copay). There are also big differences in the size of the provider network, so it makes sense to check your preferred physicians (if any) and hospitals.
The thing I'd be very wary of is things like "50% coinsurance after deductible" which I think translates to "this is catastrophic coverage, you're responsible for all 'regular' medical expenses and we'll cover things like hospitalization."
None of the selection is easy, even for professionals (https://armandalegshow.com/4-why-you-and-i-will-likely-pick-... but all of the shows are interesting). Still, if you're in one of the states that allows a little longer to get on an Exchange plan and you need one, do so.
Emergency situations are exactly what insurance is for. Emergencies account for a minority (<15% IIRC) of health care spending.
Nobody advocating for free market healthcare is expecting people to shop around in emergencies. People are expected to shop around for good insurance plans which will cover emergency situations to their satisfaction. That is why many free market healthcare supporters also support removing the incentives for employer-provided insurance plans:
- remove the tax exemption for employer-provided insurance
- add a tax exemption for individual/family insurance, including a rebate for the amount of money payroll (social security and medicare) taxes would affect the amount of money available for that insurance
This way, people don't lose their insurance when they lose their job, and people have more insurance options. This would also likely have a beneficial affect on insurance competition.
"That system" as described by parent has not been tried, at least not in recent memory. What we see happening now are thousands of unintended consequences from government meddling with the free market.
I think you mean from the "free market" - which is neither free, nor genuinely a market - usurping the good-citizen responsibilities of mature and sane government.
Proper insurance pays you for insured losses you incur.
When my car is damaged in an accident, I take it wherever I want to have it repaired. I don't have to think about whether the shop is "in network" or not. My insurance pays for the cost of the repair, up to the limits of my coverage. Simple.
I'm not sure if you have ever done this but there are a lot of caveats to that. Many car insurers will have you shop around for a good price, have you pick one of their preferred repair providers or may decide that damage you claim happened in the accident was preexisting. The job is called "claims adjuster" and I'd be surprised if no one from the insurance company visited you when you filed a claim.
Is there any chance that facilities that don't "accept" my credit card would be able to:
* Not inform me they don't accept my credit card
* Provide the goods and/or render the services
* Charge my 10 times the standard price for those goods and/or services because my card was not accepted?
No sane person would agree that this would be an acceptable regime for credit cards. Yet it's the world we live in with health insurance.
A "free market" is only effective with price transparency and discovery mechanisms. This is not possible in the current healthcare and insurance system as it exists today.
---
Aside from that, you failed to even engage or address the following points from my earlier comment.
> Further, even if the facility you visit does accept the insurance, that's no guarantee that all doctors within that facility accept that insurance.
> Even further, there's no guarantee you'll be conscious to validate that you go to a facility that accepts your insurance.
I think both of those points address and rebut your "check who accepts it" argument. Do you have any response to those?
If you read the article you'll find that the problem is that while the hospital may accept your insurance, a particular doctor won't. Also for some reason some doctors don't even know what insurance programs they'll bill.
...because even if you end up at a hospital where your coverage is great, they often have doctors or providers that won't accept your insurance, and there's just about no way to know this beforehand.
Well I don't have any legislation on the docket anywhere, but I would fully support the complete separation of health insurance from employment compensation. It's just another layer of obfuscation between the consumer and provider in the marketplace.
I'm doing it, and a few other libertarian type people. I agree with your statement though: we are a minority. Most who call themselves free market do not see how employer provided plans make things worse.
If it's such a free market, I implore HNers to explain what it might take to start your own free market hospital in the United States. Let me know what regulations you'll need to meet. Compare to opening a cafe.
And I'm not saying a hospital or a cafe ought to be at all similar. That's not the point. The point is how odd it is to pretend that health care is a "free market" in the current state as some rhetorical device to associate these surprise fees with free markets.
At a cafe, you don't get charged for using a stirrer or spoon or napkins. A cafe doesn't charge you for sitting on a stool. Free market health care would operate in the same way, if it existed. You get charged for your operation, they don't add in fees for specific items that you needed that would reasonably be expected as part of the process (a Tylenol pill, using a tissue, the gloves your surgeon wore). And again, I'm not suggesting this is how it ought to be, but let's not be disingenuous and pretend that absurd, opaque prices are somehow a result of a free market.
> Free market health care would operate in the same way, if it existed.
Any particular reason you think that?
Cafes sell standardized products--if we order the same small latte, we get the same thing and pay the same price. If you "require" something different, you pay a different price. Almond milk, for example, is $0.50 extra, near me. Flavored syrups cost a quarter.
Medicine is a lot less one-size-fits-all. Your fractured arm could be harder to repair than mine and thus takes longer or requires more supplies (and those aren't cheap--bone screws can run $40+/each). Maybe a diagnostic test is inconclusive and needs a more expensive follow-up. You can't really know how some of this is going to go beforehand. I suppose some places could offer a prix fixe option, based on their expected cost + a safety margin. I bet many wouldn't though, because the variance can be huge.
The problem is that neither models work and both have shortcomings.
In the US model healthcare is a profit center which allow those who can afford to get help and those who can't various sub-optimal variations of help.
In the ex. Scandinavian model healthcare is a cost center and there is a set budget each year which the providers need to function within. This means that prioritization needs to happen and various illnesses and procedures are limited to x amount a year.
Healthcare is a wicked problem cause it's a good thing that it's a profit center in the sense that it provides budgets to do more research and it's a a bad thing because it makes it unreasonable expensive to to not have healthcare.
In the scandinavian model it's a good thing that everyone gets treated (more or less) the same but a bad thing that they don't have as much capital to work with invest in new machines and that there are budgets which limit how much the government will spend on various procedures.
Personally I would like the system to be so that you pay to get normal check-ups, there is no limit to how many doctors are allowed in different parts of the healtcare sector and no one goes bankrupt from getting seriously ill.
That would at least help with some sort of a balance I think.
Of course the problem is that the US is such a big country with huge immigration and scandinavian countries arent so it's always hard to compare.
> Of course the problem is that the US is such a big country with huge immigration and scandinavian countries arent so it's always hard to compare.
US Population: 325 million
US Immigration: 1.5 million (2016)
EU Population: 512 million
EU Immigration: 2 million (2016)
(taken from top Google results)
It's fairly accurate to say that, compared to the US, the whole of EU has a "Scandinavian" model of health-care (ie, states guarantee good health-care services to everyone).
You can get downvoted by sounding like a knee jerk racist. Go spend a little time looking into where healthcare money is actually being spent and written off as bad debt in the US then come back with numbers and sources. If you can back up that illegal immigrants are the source of healthcare cost issues in pretty sure we'll all be impressed.
That's not what I said at all. I was explaining how the US system is very different than the Scandinavian system. That's all. You can't compare them at all.
Whatever racist undertone you heard there was your doing not mine.
Any time you're in an online discussion of US healthcare expenses and use the phrase "11 million illegal immigrants" you've pretty much just placed yourself into a category as far as almost anyone else reading the discussion is concerned.
That may not be what you meant to do and that categorization may not be fair, but it's one of many possible trigger phrases.
Its pretty obvious to anyone who is not looking to get triggered that there is nothing racist nor fingerpointing in what i say. The illegal immigration is used to illustrate one of the things that make the us system wastely different especially from the scandinavian system even though they are always used as an example. Almost every person there is has lived their whole life there.
And given i dont actually give you any other reason to think i am racist its pretty absurd that you decide to make that interpretation of what i say but unfortunately its becoming more and more the norm. Try asking me what i mean next time instead of just throwing words around accusing people you dont know anything about for being racist.
Your comment was making an implied link between the difficulties in the US healthcare system and the 11 million illegal immigrants - whether you intended or not (if you didn't, there'd be next to no reason to bring up illegal immigration at all).
Why would illegal immigration have any impact on healthcare, unless you were implying that they were a drain on the system (which is an assertion needing to be backed up by facts)?
My comment was making an implied link between many different things, illegal immigration being one of them. As it has an impact on the complexity os the US healthcare system and is one of the reasons why you can't just have a Scandinavian model.
There is a world of difference between a small homogenous group of countries where everyone pays more or less the same taxes their whole life and where immigration is fairly limited and then a country like the US where people arrive often later in life after they grew up other places and before they start paying taxes to the system.
Healthcare budgets are built up over decades not just year over year. It's based on people when they are young and don't cost too much for the system pays to the system so that when they grow older they are offset by younger generations again.
11 million people who live partly outside the system even when they pay taxes is a big number and since they live concentrated in around 20 metropolitan areas almost half of them in 3 states that make them an actual issue on top of the other things as they are not just distributed across the entire country.
In what universe it's racist to point out that illegal immigrants adds to the complexity of why the US can't have the scandinavian model is beyond me. You are the only one making illegal immigration a matter of race for some absurd reason.
There isn't a single EU health care system. Each country still does their own. Maybe each US state could do their own, but there are huge concerns about freeloader problems since we have unrestricted movement between states in the U.S. From what I've read the systems of European countries are being threatened by the freeloader problem that increase immigration as of late has caused.
There is unrestricted movement in the Schengen area, which is a subset of 21+ states of EU for the past 10 years, with current population of 420 million people.
(8+ state for the past 21 years, those 8 states having population of 291 million today)
That doesent mean the healtcare system is the same, its not. Again you probably need to do a little more studying of scandinavia and the EU cause you are getting some fundamentals pretty wrong.
My previous Norwegian employer gave me private health care as a perk. You had to get a recommendation from a government general practitioner first, but after that, it was all private, presumably to get employees back to work faster instead of having them wait for months for an operation.
Of course, most people/companies can't be bothered with this, since the government health care is good enough, but paying for private healthcare is definitely a non-theoretical option.
Of course the problem is that the US is such a big country with huge immigration and scandinavian countries arent so it's always hard to compare.
I really don't understand why it being a big country would make things difficult. Any sane person would adjust the needs dependent on state and smaller. Norway's population is about the same as Indiana's, but is more sparsely populated - so some of the same problems as the western states. The benefit of the US being large would be that there are more pools to draw money from. And there are just as many opportunities to save money.
For example, Norway will send a nurse to one's home up to 6 times a day. For free. Even if you live on a cabin on an island or on a mountain. Why? Simply because it is still cheaper than a nursing home, overall. And as a bonus, folks tend to live longer and be happier with life.
As far as immigration goes, it is impossible to compare. But: Not every immigrant gets free healthcare. I get the state healthcare because my immigration status is family immigration - my spouse is Norwegian. If I were here for a job, however, I'd have to pay for health insurance. Of course, they'll still treat someone that pays cash and still treat emergencies. I don't really see how this would be an issue in the US either so long as the laws were set up correctly.
I'll further add that I think the healthcare is a bit different if folks are coming from an EU country - there are agreements in place about health care and things like that. Again, I don't see why this wouldn't be the case in the states.
That's because you haven't considered how big the US is and you haven't considered that the US is mostly a land of immigrants not a land of people who lived their almost all their lives for several generations.
Healthcare systems like the scandinavian are established over decades as the young needs to pay for the old until they get old themselves and have to get covered by the young.
This kind of system is more or less impossible in the US and it would be extremely expensive.
That doesn't mean the current system in the US is any good, it's horrible to say the least. But the scandinavian dream isn't possible in the US and I have yet to see anyone showing any actual proposal that would work given the setup with federal and state and what they can decide.
*That's because you havne't considered how big the US is and you haven't considered that the US is mostly a land of immigrants not a land of people who lived their almost all their lives for several generations."
I'm American. The first one is easy enough to consider. I can drive to Sweden in the same or less time than it would have taken me to get out of Indiana. I know it is big. I just don't see how that is an excuse. It isn't like you can't customize health care to a geographic area so it serves the needs of the people best. There are multiple ways to do that.
And that bit about immigration? That's propaganda 101 in school. Trust me, I'm aware. I fail to see how that is an issue. Most folks in the US aren't new immigrants: They are at least 2nd to 3rd generation. Even if I take the higher numbers I saw - around 25% - most folks are still just Americans. I don't really see how that affects anything. Don't most folks still want healthcare? Do immigrants avoid health care? Don't most of these families have at least one working adult paying into the tax system?
And of course it would be expensive - the current system is expensive. But it isn't efficient now, and that can easily be changed. Just because you haven't seen a proposal you'd be happy with doesn't mean it can't work. Most of the proposals I've seen in the US are more focused on preserving health insurance companies instead of focusing on getting health care ot everyone.
These countries are homogenous which also means politically. You will be hard pressed to find any real fundamental political differences between parties in the scandinavian countries.
They are all on the left side of Sanders.
Furthermore, it matters quite a lot that you are dealing with a fairly limited population who all suffers from more or less the same issues because they genetically are alike.
And again keep in mind the Scandinavian countries have budgets which means that you can't always get the treatment you want/need even if you had the money.
Again I am not saying the US system is good it's obviously not.
But a single-payer system in the US just isn't realistic or attractive for that matter.
The problem in the US is the price, but that price is held up artifically not because of the market. So we need to remove the things that make the price go up that hight. That IMO would be a much better approach than trying to mimick scandinavian countries as great as they are for their population (but definitely not without it's problems)
Again, I don't see the size as anything but an excuse against it. Surely in the US, it would have to be adapted to different areas' populations. I'm not convinced Indiana is so much less homogenous than, say, Sweden. They are definitely not all on the left side of Sanders.
And again keep in mind the Scandinavian countries have budgets which means that you can't always get the treatment you want/need even if you had the money.
I don't know where you get this sort of information. I will never not be able to afford my medication. I broke my arm and got immediate, affordable treatment and had paid time off work even though my job was seasonal. In the US, with insurance, I would have struggled, not only with hospital bills, but with work. If you have an issue that they cannot treat in the country, you can travel outside of the country for treatment. Even if you are poor and have no money - the state does that. There are private hospitals and clinics around - if you have money, you can use them. They aren't always that much more expensive and the waiting period for non-emergency stuff is less.
The bottom line is that you are against a single payer system. That's fine, be honest, but please make sure your actual facts are facts instead of things people hear.
It sounds like you don't want to see the problem which makes it hard to have any discussion.
The size is a problem given that you would need to be able to offer consistent care across the nation this is exactly the kind of problems that single payer systems deal with. They are an actual problem in the scandinavian countries and these countries are small. Federal is federal.
I am not against a single-payer system. I grew up with one as I am Danish so I want a single-payer system. Especially as I have been having 2 melanomas and might likely get more and live in the US. I just wont work here and I won't be able to get the kind of care that I get now.
I know both systems pretty well that's where I get that information from I been living in both and experienced both.
> This kind of system is more or less impossible in the US and it would be extremely expensive.
That's literally how Social Security works, and the fact that more guest workers pay payroll taxes into the system than are eligible to collect benefits from it actually makes it slightly cheaper than it would otherwise be.
That's how social security works and it works great in countries with little immigration not in countries like the US where there have historically been.
I think it depends on the job. If you work for a foreign company and are temporarily in Norway (e.g., spending a quarter at the Olso branch from your HQ elsewhere), you're on the hook for your own insurance: https://helsenorge.no/bo-i-utlandet/posted-workers-outside-t...
Another thing to keep in mind is the Scandinavian countries are resource rich with comparatively low populations - Norway has oil, Sweden has timber and iron ore, Finland has timber, etc. These helps build excess in their budget
I think everyone acknowledges the current system is the worst of all worlds. _Both_ the left and the right are correct in my view: (1) single payer universal healthcare or (2) removing a ton of the existing government regulations and forcing healthcare to behave more like a free market, would each be better than the existing system.
I don't think "free market healthcare" is oxymoronic though. It does not seem to me impossible (logically...maybe it's impossible politically) to remove the current incentives that prohibit price discovery and/or enact laws and regulations that incentivize it.
Legislation requiring up-front presented costs to be honored and any additional procedures/costs to be cleared with patient consent as they happen (or a consent waiver obtained from the patient with a promised limit or incentive such as overall discount) might be an improvement. Or it may increase costs for the worse. Who knows.
Careful there though. If a surgeon is operating on cancer and discovers that the tumor is much larger than expected the operation will take longer - be more expensive - or the surgeon does the operation as planned and then charges even more for the second surgery to remove the rest. Or maybe all operations are estimated as the worst case and so you end up with no more clue about what you will pay than today - in some imaginable worst case this could be a five million dollar operations, so even though 99% are only fifty thousand you get that high estimate.
Which is to say don't propose something until you understand the unintended side effects. You can get your desired result but while making everything worse. (this paragraph applies to everything in politics)
I mean, I guess, but that's kinda a worst case. My vet, for instance, quoted me up front, made me sign to say that I was willing to pay (I think) up to $x000 and notified me that they might contact me if they need to do extra work, and then did the surgery with an up front payment. They ended up refunding me money after the fact.
No reason we can't have something similar that in US health care as far as I'm aware, at least for the happy path where the patient is lucid and in a reasonable state of mind up front. But then again, why do we have to worry about this when plenty of countries have a basically-zero-fee system in place?
That’s not really the problem we face, though. Our problem is you ask how much it costs to give birth at a hospital and then everything goes according to plan and later you get endless bills for much more than they said, often from providers who weren’t even in attendance, for materials that weren’t even used, and so forth.
> Which is to say don't propose something until you understand the unintended side effects. You can get your desired result but while making everything worse.
I think the American experiment in trying to provide market health care has demonstrated that you can, in fact, have a 'free' market for healthcare, while making almost everything about that healthcare worse.
A constant 30% discount on employer insurance via tax breaks does not explain the ludicrous growth in hospital bills over the last 4 decades.
Your vision benefits enjoy similar tax breaks, but I've yet to see an optometrist try to bill someone without benefits $800 for a vision exam, or $4,000 for a pair of glasses.
Insurance companies benefit from all those tricks: medical care billing is too complex to understand unless you have a full time team of people to understand it. Insurance companies have this team and you don't.
Vision doesn't work that way because enough people don't have basic vision care that they won't stand for the complexity.
NO, the problem is medical billing was allowed to become too complicated, and it is very hard to unwind that situation.
I'll contend (though of course there is no way to prove this) that if we hadn't had the advantage to company provided insurance the complex billing wouldn't have developed in the first place.
I’m reminded of airports which function very similarly to healthcare. There’s absolutely no choice of merchants I can be in an airport is decided by a very small group of people. It’s not like an open air market you’re finding some developing countries where people can just set up shop and start selling stuff. It is a tightly very tightly controlled market I have very very small number of entities and organizations.
frequently couldn't reasonably be expected to refuse service even if they did believe it was overpriced
I wonder if private urgent care businesses could offer free rides from emergency rooms to other facilities? There might well be laws against this. However, the existence of such services might give people a degree of choice they don't currently have.
A few years back, I was in the position of seeking emergency room/urgent care services for my girlfriend at the time in North San Jose. It was not a pleasant experience, to the point where we just decided to simply give up. On the other hand, I did the same for my girlfriend at the time in Houston, and found the whole experience to be relatively smooth.
Even if you could flip a switch and go to a free market, that doesn't reset where the current players are, so they will use that going in to insulate themselves and abuse the market.
For pricing, Hospitals/Insurance Co.'s are unwilling to absorb the cost of the statistical chances that something goes wrong or extra labor/things are needed during healthcare. That's why the patient-facing price could be anything and you get an itemized bill.
The only way to get slow-moving and predictable patient-facing prices is to get the hospitals/insurance to absorb these costs.
I was a victim of the surprise out of network bill in the Portland, OR area. I did all my research before hand: hospital in network, surgeon in network, etc. but ONE person in that operating room was not in network and SURPRISE i'm out thousands of dollars. The worst part about this is my state passed a bill to stop this prior to my surgery, but the bill's effective date was roughly 3 months later. Talk about bad timing.
I'm at a loss as to why the US is still dead set to have no meaningful health coverage.
I got burned by this in California a decade ago. A dentist charged me $4,500 to fix a broken tooth (panic!) and fill in a cavity on a Sunday.
Had I known then what it might have cost I'd have simply flown back to Europe in the next flight ($600-800 at the time) and get the same thing done for under $100-200 with a full refund from my local social security.
Adding insult to injury I had a very expensive international health insurance policy owing to my traveling around the world back then. And they didn't cover dental with my plan. I knew they wouldn't. But it was still mind boggling to me in that I never expected a casual procedure that would have cost me €150 at most anywhere in Europe - most of which would have gotten refunded at that - to cost me a whopping $4,500 in the US.
The health insurance industry spends millions in donations to politicians on both sides. So, the reason we have a poor health insurance industry is money.
There was a story about an Indian guy - he flew all the way from California, spent two weeks in India, took a bunch of MRI etc scans and went back. The entire of the trip, including airfare, hotel, scans etc was less than the cost of a scan in the U.S. Not sure how much of this is true (and yes, I do realize I shouldn't be comparing US with a developing country like India, cost wise), but it is definitely believable.
Given Theil's penchant for SnowCrash style Rafts, I'm surprised he hasn't parked an old oil tanker in international waters just off LA, retrofitted it for outpatient procedures and a helipad.
There is no political will to subsidize healthcare if the health costs themselves arent fixed
This second aspect has never been addressed on a national level, or barely at all.
At the state level, if you think of them as their own countries some do have very accessible programs. Some even having universal healthcare in that state.
So the US is complicated.
And then there is the distrust of how people of other cultures in our country would use a subsidy if it isnt clear that they have the same ethics and motives. This exacerbates many political issues.
>I'm at a loss as to why the US is still dead set to have no meaningful health coverage.
The US isn't a monolith. The majority of the population very much wants meaningful health coverage, but thanks to Supreme Court decisions like Citizens United, corporations are entitled to free political expression under the first Amendment, so they can give unlimited amounts of money to political candidates. This allows uberwealthy individuals to form corporations for the explicit purpose of installing anti-taxation cronies into legislatures at both the state and national level.
Our political process is very corrupt, and it's taken a national emergency (Trump's Presidency) to wake people up. The 2018 midterms demonstrated that far more citizens are paying attention and plan on voting, so hopefully the US goes single payer soon, but it's going to be a brutal political fight.
advertising is the biggest thing 'educating' voters, and usually it's usually something along the lines of here's why <party> <candidate> is bad, vote for me instead. News media is trash and unreliable as they too pander to advertisers or are just spewing nationally distributed talking points.
Bernie who was the most vocal about changes was taken out by Hillary, but no one batted an eye. No one really wants change to the healthcare and pharma industry as it will hurt the entire ecosystem (especially advertising $).
USA dentists don't work on Sunday. If you had waited until Monday you would have had many more options. Besides what could she have possibly done to "fix a broken tooth" in one day? Nobody was milling crowns in the office a decade ago. If it was really just a filling, wow.
Do dentists in Europe work on Sunday? In my experience the grocery stores aren't even open...
I've had emergency dental treatment in an NHS hospital in the UK for an extremely painful dental abscess - was treated first thing on a Sunday morning.
> I've had emergency dental treatment in an NHS hospital in the UK for an extremely painful dental abscess - was treated first thing on a Sunday morning.
Emergency dental care is provided in the US as well. Filling a cavity is not considered an emergency.
Very few oral problems are emergent. GP's abscess would have been visible on examination for months, and certainly was uncomfortable before it was extremely painful. In many cases the first treatment is a course of antibiotics, which any USA ER could administer perfectly well.
"certainly was uncomfortable before it was extremely painful"
Actually it wasn't - went from nothing to blinding pain as if someone threw a switch. I'd have 10-15 minutes of agony then it turned off for the same time and it repeated at that frequency all of the Saturday until a GP came out on the Saturday evening and gave me painkillers and told me to go to the emergency dental clinic the next day.
It was right in the middle of my 3 years exams at University - which was a bit of bad timing!
Hah, there's not a dentist in my entire County that works on Friday either. I've been in the situation where I've called each and every one, all closed Fri-Mon.
Even here in Norway, even on a Sunday it wouldn't have cost anywhere close to USD 4500. I have asked colleagues in the US about the cost of dentistry and most of it even when booked in advance is noticeably more expensive than here. But of course here we have full transparency, I can shop around.
Exact same thing happened to my friend. He did all his research, and while he was under anesthesia a nurse assisted that was out of network. $5k out of pocket. He ended up getting it removed after some run around between insurance and the hospital.
People misunderstand non-profits. There is nothing stopping you or I from starting a non-profit and soliciting donors then paying yourself a $1M salary.
Non-profit simply means any surplus of revenue is spent. So, the more revenue generated by a non-profit's paying customers means they get to funnel that to their core mission (likely research, possibly those that can't pay, or cynically more salary for those running the show).
Definitely not paid for with reimbursement revenues.
> amenities for staff
Try cutting these, and see how quickly 1199 SEIU comes down on you.
> raising administrator salaries "to retain premium talent", etc.
Even if you assumed that there were no relationship between the wages paid and the quality of work performed (there is), these are nowhere near big enough to account for the difference. They're also not that far out of line with other countries, either: 25% in the US, compared to 20% in the Netherlands, for example.
But more so than that: they're SG&A expenses, which are further down the balance sheet than the reimbursement revenues. And yet, hospitals actually lose money on the top line for Medicare patients (who represent about 40% of the market). That's the real reason reimbursement rates are raised for private insurers - the private insurers are required (by law) to pay more, and they need to subsidize the sub-COGS reimbursements from the public insurers (Medicare, and to a lesser extent Medicaid).
So no, none of the things you listed actually explain the reason hospitals charge private insurers the rates they do.
> No. That’s the justification given so that people get angry at the wrong thing. Hospitals charge this because they CAN. They are doing what businesses do and that is maximizing their profit.
Hospitals make very low profit margins; hospitals have been hemorrhaging money and either being bought out by hospital systems or insurers, or even shutting their doors entirely.
In any case, it's not uninsured patients that cost the hospital money; there aren't enough of them to make a difference at most hospitals. The patients that cost hospitals money are Medicare patients, because Medicare reimburses rates that are below COGS, and private insurers are required by law to reimburse more.
In other words, yes, it's the politicians that enable a broken system, but no, it's not the uninsured patients who are at fault, and it's not "profit-maximizing businesses" that are at fault either. Hospitals don't want this convoluted billing system any more than patients do, but it's literally forced on them as a result of accepting Medicare patients.
For this reason, I'm beginning to think that we do in fact have "universal" healthcare in that anyone can turn up to the hospital and be treated despite their income. For those who don't pay (or don't have insurance) the hospital spreads that cost out over their other patients and likely marks up the price to insure against non-payment. So we end up with an unregulated mess where any one hospital has to insure themselves (in the form of passing on costs) against the percentage of patients that will simply never pay.
Given that this is going on, why not just switch to a single payer system and spread this out over a much larger population rather than each hospital trying to insure against it?
We have universal care for emergency treatment, and only to the point of stabilization, and in a manner that basically combines all the worst aspects of various systems.
You can't get months worth of chemo or physical therapy or dermatological consults or whatnot at an ER.
This is actually only a half truth. Emergency rooms are required to treat patients who need emergency care. They don't need to fix all ailments. If you have cancer they can turn you away, but if your organs are failing as the result of cancer they have to treat you. If you need a heart surgery they can turn you away, but if you're having a heart attack they need to treat you. For the most part, treatment is pretty much just making sure you're stable and can leave the hospital without immediately dying. This only applies to emergency rooms as well. Where you go to get surgeries is usually not the same place you go to treat an emergency condition. It might be affiliated with the same hospital, and might be attached to the emergency room, but it isn't itself an emergency room.
Today is "don't believe the comments day" it seems. How is an unconscious person meant to be stop an "out of network" nurse assisting? Is there a tattoo that you can get?
> How is an unconscious person meant to be stop an "out of network" nurse assisting?
They can't. That's the problem - there's little you can do to stop it from happening, even if you're aware of this sort of billing problem and try to take steps to prevent it.
> Surprise bills occur when a patient goes to a hospital in his insurance network but receives treatment from a doctor who does not participate in the network, resulting in a direct bill to the patient. They can also occur in cases like Calver's, where insurers will pay for needed emergency care at the closest hospital — even if it is out of network — but the hospital and the insurer may not agree on a reasonable price. The hospital then demands that patients pay the difference, in a practice called balance billing.
> The surgeon's office later told her that he belonged to two different medical groups. One was in Morgan's husband's health plan network, the other wasn't.
> The surgeon's office later told her that he belonged to two different medical groups. One was in Morgan's husband's health plan network, the other wasn't.
I got this one, it was mindblowing. For ER work, they'd bill through one practice, for scheduled appointments, another.
I got balance billed for $11k. My father, who worked in employee benefits for over 30 years, couldn't even figure out what was up at first. Then they filed to send me to collections because I kept refusing to pay (note, I'm in California and this billing is illegal for life-threatening emergency visits matching the situation I was in). Finally, the insurance company stepped in and covered me, but we were only able to achieve this because my family knew people personally at the insurer.
With Medicaid (in New York, at least) a provider isn't allowed to bill a beneficiary for treatment. It is such a huge stress reliever. I can't figure out how so many people continually fall for the propaganda against single payer / Medicaid/care-for-all.
From what I understand (which is honestly not much), I think in cases like this you can contact the hospital and just insist on paying the same amount your insurance would have paid, and they'll often take it. That's just what I hear, though.
This is horrible advice. Do not agree to pay a penny of that fraudulent bill. If you didn't agree to the service, you should not be liable to pay.
Call the hospital and demand it be removed from your bill. That's what others[1] (including myself) have done and the fraudulent charge was eventually removed.
The absurd part is that you would even need to do this. How many people don't understand you can fight healthcare charges and get them removed? How many have the free time that it takes to call the billing department over and over?
The whole health insurance system is trash and needs to be replaced.
My last visit to a hospital it was requested I arrive 30 minutes early to "fill out paperwork". After arriving at the radiology department an office assistant took me into a nearby room and had me sign consent forms and make payment on the spot. Anxious for my exam I signed everything and handed over my debit card. Later on I realized one of the forms cemented acceptance of the debt and guaranteed my full payment of it. If I chose to I would have very little ground to stand on disputing the costs ($800 for an ultrasound).
Hospitals are for-profit entities that will optimize debt-collection and bargaining power over patients. They will start taking payment upfront as well as influencing patients to choose financing options that are in the best interest of the hospital and not the patient themselves.
It's hard not to feel like the whole system is rotten.
Yes it is, there are several factors jacking up the price in the US. There are some good videos on it on Youtube. I was always wondering why people think that it is a free market there. In Europe there are several countries that let you use private and public health insurance (even at the same time) and you can go to any healthcare provider and still get a reasonable price. In my country the private provider "industry" is booming and most lab work can be done in a private manner, usually for a very reasonable price. Most of this is accessible in a week ahead booking time.
Regardless of insurance, when you offer to pay cash hospitals will often slash the price considerably. If the hospital has to use a debt collection agency, then they're looking at getting a small fraction of the list price back - sometimes an order of magnitude less. They're willing to negotiate accordingly.
Not in all cases - it varies significantly for everyone. In my case the hospital, surgeon, anesthesiologist, and some of the assistants were all billed under different systems and as separate entities. The hospital has nothing to negotiate because they're in-network so I had no balance due (meet my out of pocket maximum).
The surgeon's assistant was the out of network provider and he was also part of a different practice, so it was his practice billing department that would not budge because they deemed their costs as reasonable and "already discounted".
Yes, moonlighters (the surgeon in that room) are expensive (to both you and the hospital). Why do you think that person wound up there?
Otherwise underpaid, overworked surgical residents leave either due to truly catastrophic burnout, mental illness, family emergency or pregnancy.
They are replaced by moonlighters, because the economics of the surgery are that the nurses and other unionized employees get mandatory breaks, so the seemingly 1-2 hour delay waiting for a different resident to be free balloons into a multi-staff scheduling fiasco. We could amortize all those costs into "surgery minutes" which are paid whether or not the literal room is in use or whatever.
It's a math problem if by saving surgery minutes, the hospital saves real economic money for itself, the patient or the state, so I'm not sure if that is or is not the case in your particular case.
What's interesting isn't that there's legislation one way or another, or that you feel like you got a raw deal. The legislation isn't going to change what it says it will, because it will still make sense to hire moonlighters. And motivated people like you will still somehow still wind up paying the cost.
The real test of your merit is whether or not you think in the grand scheme of things, this is fair. Are you frustrated that there may have been a pregnant resident, and that's why there's a moonlighter in the operating room?
What does justice look like there? Cut you a check for thousands of dollars? That never happens. Retribution on residents who might get pregnant? That's what happens.
Your situation is shitty. I know in most movies, books and the press, the doctor is usually the antagonist. We live in a world that resents their disproportionately immigrant backgrounds, disproportionately even gender balance compared to other professions, and most of all their pay, despite their hard work. How do you feel?
Except I highly doubt the staff and doctors are actually being paid in proportion to the charge. I doubt they’re even being paid a significant portion of that bill. We’re not hurting doctors and nurses when people claim to want more efficient healthcare strategies. There are ways to allow moonlighting, such as everyone being in-network to a greater social healthcare system.
Even out of network, you are able to bill your insurance directly. There are a lot of private practices not in network with any providers at all where insurance will still cover, you just have to do the legwork yourself usually.
Appealed twice and both times they denied it stating I didn't require the surgery despite the fact they pre-approved it and paid for all the in-network costs. I ended up paying it because I had the money and I couldn't handle the stress of a legal battle (which given what I've read is an uphill battle).
Sorry to hear that.. you can usually appeal up the food chain sometimes.. e.g. to your states insurance department if the plan is regulated by your state. And at the Federal level you can also submit a ERISA appeal. None of it is fun and then there are deadlines... Also if you are on an employer provided insurance plan, you can talk to your HR who will have an insurance rep who can sometimes make these things go away e.g. get them paid. If you are at a large employer that self insures and uses a third party admin (like Cigna) then they can tell the admin to negotiate with the doctor/hospital and pay it.
I'm not an advocate of government paid health care, but hospitals and medical providers should see that this train is coming and if they don't become more transparent it's going to be forced upon them.
I don't have a problem with ER care being more expensive -- that isn't necessarily unreasonable when you are getting care in an expensive facility open 24x7, fitted out with equipment to handle any possible medical emergency, and staffed with highly educated people who make a lot of money. But it is unfair to have no idea what costs you are facing and whether any of those costs are out of network on your insurance.
> But it is unfair to have no idea what costs you are facing and whether any of those costs are out of network on your insurance.
It's practically impossible to make an informed economic decision about truly emergency medical care without heavy regulation. It's not uncommon to be literally unconscious while all the care decisions for you are being made by others.
See this article for an example: some uninsured woman had a brain hemorrhage and woke up with $357,000 in medical bills:
Both my kids were born early. The medical bills for both totaled (with hospital stays for babies and mom) north of 100k each, the second WAY north.
Both involved situations that were "emergency" type situations. We couldn't shop around, we couldn't even sign anything. We trusted the hospitals and doctors and went from there. Fortunately I had good insurance, if for some reason I had to pay it would have been a huge financal burden for years and years.
And let's say I did have time to think about it? What then? I'm not a doctor, this isn't shopping for a car... I don't feel like I could possibly know enough about emergency baby birthing, surgery, etc to know... "Gosh honey when the baby's heart rate starts to slow unexpectedly, I think we should save a few bucks".
I think pregnancy and labor is what's going to finally break the camel's back.
Having children is a pretty basic part of being human. And the costs are such that even millionaires are going to feel it. When basically nobody can afford to participate in reproduction, something is going to go sideways.
With my "good" insurance, I still ended up with a multi-thousand dollar deductible. Which I thought was problematic until I started hearing about people who have high deductible plans that only make you pay 20% after hitting your deductible.
For a 100K bill, 20% is still absurd and especially after you've already paid $2-10K out of pocket.
Usually coinsurance is limited by an 'out of pocket maximum'. So even if something happens where you end up with like 600k in medical bills the most you will pay will be like 8-20k (depending on in-network vs out of network). Which is still insane but not as scary as six-figure medical bills despite being insured.
One issue with describing figures like 600k is that I think the medical industry has a lot of funny money running around. The doctor somewhat arbitrarily charges 10k to the insurance company, insurance disputes, the doctor hires a lawyer who takes 30% of the negotiated outcome, and negotiation finally ends up at $2k.
The patient sees a $10k bill, pays a $300 deductible, and only $2k ever actually materializes in the exchange between doctor/insurance. And afaict, this is the expected operation.
Of course, when you're uninsured, the numbers stop making any sense, because they fail to go through the convoluted process that reduces it. You just get the $10k bill and thats the end of story. But for the insured, a $10k bill is not $10k exchanged.
Yeah, some of the explanation of benefits I've received are insane. Insurance is apparently able to negotiate ~50% bill reductions for multi 10K bills.
Dealing with Indians, the normal bargaining tactic is apparently start with like 300%/10% of the expected, and end up at 110%/90% as anywhere else would. From America, starting is 120%/80% or so. Totally confounding when you first start negotiations, because they're offering these absurd numbers as if its normal..
I think the same culture exists with doctors/insurance. It's not that they're skilled enough or have enough power to negotiate down 50%... doctors are putting numbers up expecting to be reduced to 50%.
And then us poor saps get slapped with these absurd numbers and thank the gods we had insurance... but no one involved ever really expected to pay that number. And ofc, without insurance, you're like an american trying to shop in india -- no idea how to play the game, trying to negotiate in the american fashion with 120%/80% when the other guy started with 300%, and don't have the information to realize that initial $20 offer negotiated down to $18 isn't even close to what an indian would have managed (probably $5).
And its not like he's going to correct you when you fail to negotiate properly.
> Which I thought was problematic until I started hearing about people who have high deductible plans that only make you pay 20% after hitting your deductible.
If I'm not mistaken, those plans also have an Out-of-Pocket Maximum. So you pay 100% up to your deductible, then some fraction of the cost above that until you hit the OOP max.
Considering she was unconscious she could not possibly have consented to those transactions. What laws exist that allow these companies to unilaterally create these transactions, and what limitations do they have?
They have literally no limitations. The reason that an advil at the hospital costs $200 is because they were afraid if they made it cost $20000 people would burn down the hospital.
There is an out of pocket maximum of $7350 for 2018(going up to $7900 for 2019) for ACA compatible plans. Many plans have lower out of pocket maximums too. The health insurance company will negotiate and generally pay substantially less than $377k for a $377k bill.
On the flip side, what laws exists to say a hospital can't treat any unconscious person since they can't consent. Damned if you do, damned if you don't.
> I would imagine regulation is a lot of what stops competing on price like everything else.
Say again? Unconscious people don't have the agency to make price competition work, regulation or no.
You need to be conscious to comparison shop. You also need lots of time to do so, time you don't have when you're having a heart attack or bleeding out from a severe injury. Regulation isn't the problem here, it's the lack of the right kind of it.
Being conscious or not has little to do with inability to comparison shop for healthcare in general. I wouldn't disagree that what you're talking about should be illegal and I would expect it to already be illegal.
I was not an advocate for gov't health care, but I am now for the same reason you stated. I have a high deductible plan, and have tried to get quotes in advance, but never can. I have been ripped off multiple times, despite trying to do my research, etc.
My wife is a doctor, and at this point, I think single-payer is the least bad option.
I find myself in the same boat. I've spent more from my HSA this year than I put into it (and I put in $6900) while I'm nowhere near hitting my deductible ($6K) because for whatever reason the insurance only thinks I've spent $2.7K. During this time I've tried to shop around, find the least expensive option (none of my medical needs this year have been urgent) and it's been impossible. Nobody can tell me. "You'd have to talk to our billing department, and they probably can't tell you anything until the doctor is finished."
I am now firmly in the single payer camp. Medicare for All, I guess. To the insurance companies and medical billing industry, and even doctors, I say: "Sorry, not sorry, when this train comes through try to remember you did it to yourself."
For the record, this is exactly how I feel. They did it to themselves. I really believe in free markets, and I really see the downsides of gov't intervention, but my direct experience with this particular market says we'd be better off with the gov't.
Correct me if I'm wrong, but Medicare-for-All is just public insurance. It's not a state take over of all private hospitals.
But instead of negotiating a price with you, the hospital will be negotiating with the state. Hospitals can still compete on prices and likely the state will grant contracts for non-urgent services to the cheapest provider..
Modulo, whatever level of free choice is left and what capacity is available, etc..
It’s effectively a state takeover, as providers can negotiate with the Health and Human Services department in the same way that my child can negotiate their allowance with me.
Disclaimer: In full support of single payer/government managed healthcare
Not really, you could very well imagine private hospitals bidding against each other to win a contract on providing ER services.
With penalties if capacity or quality suffers by objective standards.
(Isn't this how most government contracts work)
It's not like there is any competition right now? You can't even get a price quote for elective surgery.
Also I wouldn't be so sure that your children don't have significant leverage over you, hehe :)
(They probably don't realize how much leverage they have)
Your current experience is of a highly regulated system with dwindling options and a lot of unintended consequences that weren’t thought through with the existing regulation - it is more similar to socialized care than the free market.
Do any doctors actively campaign to change these billing practices? Bogleheads.org seems to have quite a few Docs that post there, and the attitude is mostly "I went into medicine to practice medicine / Gee, I don't bill at all, I leave that to the hospital" and other great flippant attitudes. Probably a poor community to judge the standards of medicine by as it's mostly a 1%er forum that happens to have some good advice, but that's the only exposure I have outside of my 5 minute $400 visits with specialists.
You'd think they'd be a bit more invested in the process of healing, but I haven't found much evidence of that. I hope I'm horribly wrong here.
My wife is a pediatrician at a large research university/med school. She is totally uninvolved in billing. She has no idea how much anything costs. She is aware of it as an issue, but its a giant organization, and the reality is she isn't going to try to fight the power.
Personally, I don't think doctors are the answer. I used to really like the idea of high-deductible. But eventually, I just came around to the idea that only the gov't can fix it (with lots of tradeoffs in that fix, obviously).
Not enough people actually tried to do what you did, so the high deductible plans didn't provide the desired result.
I think they could, but more people would need to be in them and try to do what you did. It needs to be enough people to eliminate the problem where insurance companies like the system being too complex because then you use them instead of paying for it our of pocket.
High deductible health plans are close to half of all policies now (in 2017 it was 43.2% according to the CDC).
Insurance companies clearly have nothing to worry about. I might be able to put in extra effort to negotiate my costs down by paying out of pocket, but then it would not count towards my deductible or out of pocket maximum. Even with HDHP, I am still clearly incentivized to just pay whatever the insurance company thinks I should.
It's a great racket to be in, really. They can negotiate the pricing in advance so that they appear to be useful in making my costs lower, while not actually incurring any costs other than paperwork. They hold all the cards and they have captured the regulatory authorities.
The problem with single payer is that it results in shortages. Look at waiting lists for the NHS, especially for mental health or routine surgery. That is a direct consequence of single payer. An unpopular view, but it is a fact.
I live in a country with single payer (Australia).
I've never had to wait for an elective procedure because I can choose to privately pay for care on a schedule more convenient to me. I have private health cover which tries to compete on this basis.
But if I had any emergency needs, then I'd be treated immediately at any hospital by the public system, which I pay into with taxes. And the waiting list for those elective procedures, if I couldn't afford private care, is a priority list - based on need.
The idea that shortages don't exist in the US is absurd - sure they do, you can't afford critical care then you just don't get it. The US waiting list is infinite.
I am skeptical of a causal relationship there. In the United States, approximately 2/3 of healthcare costs are already borne by the government. My parents are both enrolled in Medicare and they are very satisfied. Why would it not work if we just dropped the eligible age for Medicare to zero? Hasn't this been extensively studied recently?
In many cases, Medicare doesn't even cover the actual cost to provide the service. The providers make up the shortfall by charging other patients more - including charging uninsured patients a LOT more.
So if everybody was covered by Medicare, either the providers would be going bankrupt left and right, or the Medicare reimbursements would have to rise - i.e., the price to the government would increase, and the only thing to do about that is to pass it on to the taxpayers.
It's a common misconceptions that Medicare is more efficient than commercial insurance, because on paper it looks that way. But in fact they're hiding their administrative expenses by forcing the providers to do much of their bookkeeping. (Source: my wife used to manage the department in the hospital that did that Medicare financial stuff)
That is a pretty bold claim, can you cite someone more authoritative than your wife?
Kaiser, who has a plausible claim to expertise in this field, puts the overhead cost of Medicare at 2%. The raw number is more like 1.4% but Medicare does get to piggyback a lot of the administrative workload on Social Security so perhaps that is why Kaiser's number is higher.
Insurance industry advocates, who are incentivized to provide the lowest number that can be defended, put private insurance overhead at 17%.
The rest of your suggestion -- that Medicare doesn't even pay for the actual cost of service -- is hard to really reason about accurately. Prices and costs are so completely distorted now that I am very skeptical of anybody's estimates of 'actual value.' Things will change dramatically if we eliminate the insurance industry and medical billing field.
Having just experienced first world level healthcare in another country and paying for it out of pocket at 1/20th or less of what it runs in the US, I am certain we are getting shafted.
Kaiser, who has a plausible claim to expertise in this field, puts the overhead cost of Medicare at 2%.
This is exactly what I'm talking about. I'm sure that number is accurate, if you're looking at Medicare's books. I'm telling you that when you look at the way Medicare forces the industry to handle their charges, it makes the industry much less efficient, both in terms of administering the provision of care to Medicare's "customers" as well as more generally across how the industry handles its accounting in general.
Every hospital (and skilled nursing facility) has a small team of people whose job is to compile the statistics that Medicare demands, and report it annually in what's called "The Medicare Cost Report". Add up 1 or 2 or 5 FTEs across every hospital and SNF facility in the country, Medicare's claimed efficiency is quickly turned upside down. There is some work that providers have to do for other payers, but its scale doesn't approach the order of magnitude of what Medicare forces. This isn't a matter of opinion (like my wife's); this is absolutely factual and objective.
It gets even worse than that. Because the care paid for by Medicare together with that of Medicaid (which is a separate program, but rides on Medicare's coattails for a lot of its reporting mechanics) dwarfs any private payer, hospital information systems (at least the parts that deal with finance) are structured around the way statistics need to handled for Medicare. That squeezes out the ability to do any more traditional cost accounting. This is the reason that the fee for a given service varies so wildly from hospital to hospital: because they're not doing normal cost accounting (but instead tracking Medicare statistics) the don't actually have a good idea of what any given thing costs, so their fee schedules are all over the place. (I'm generalizing here, there are hospitals that do it better, but my anecdata from hospitals we've had close association with show that this problem is quite widespread.)
> Things will change dramatically if we eliminate the insurance industry and medical billing field.
It's important to note that this industry is a complete bullshit industry with complete bullshit jobs. Their only job is to say no, to stop money from going out of the insurance companies, in any way possible. That is their entire purpose.
Your medical insurance money props up this industry. Every person working in this industry and receiving a salary, and every person owning shares of companies in this industry receiving profits, are taking money that should have been spent on producing healthcare for themselves.
So however many billions of dollars of revenue this industry makes, we would instantly save most of it by getting rid of this industry.
> Having just experienced first world level healthcare in another country and paying for it out of pocket at 1/20th or less of what it runs in the US, I am certain we are getting shafted.
We are, but not by insurance companies. Their profit margins are thin. The issue is hospitals.
Sarah Kliffs idea to reduce the cost of hospitals is price controls: for the government to tell them they cant choose a price, and to ban them from accepting other insurance.
This should be a highlighted comment in this discussion. My dad just retired and shut down his medical practice. He hated Medicare as a doctor (OK, my words, not exactly his), but now that he's using it as a patient he can see why people like it so much. It really isn't going to work like it does now if it becomes the only option for everyone.
I've heard the 2/3 number (sometimes a little less, most recently slightly over, 68%) from a few reputable sources recently. At the same time, I generally consider Kaiser pretty reliable. I think the discrepancy comes from what is being included in the total -- all costs, direct payments only, tax subsidies, etc. At least from what research I've done.
Even if we take the value to be 50%, my point stands -- the gov't is already heavily involved in funding healthcare in this country. Implementing single payer at this point would simplify quite a lot of bureaucracy.
Medicare has 30 million patients and costs about 3% of gdp. Multiply by 10, and you would need to almost double the tax-base to pay for medicare.
I propose the other thought experiment: why doesnt medicare just compete in the market with other insurance plans: it charges X and provides the service. If its truly more efficient it will beat all the rest.
To really hammer home the point here, that Conservative government, in an effort to make immigration numbers go down set immigration rules to impose a minimum income for jobs that could recruit outside the EU. That minimum was lower than the government austerity cut maximum pay for nurses. Result: can't hire non-EU nurses, shortage worsens. Waiting times increase.
Eventually, as this started to be more widely known the Conservative government "fixed" it. Not by paying nurses more, not by lowering the immigration income requirement to match what they pay skilled workers like nurses, but by specifically exempting nurses.
>have tried to get quotes in advance, but never can.
>I have been ripped off multiple times,
>I think single-payer is the least bad option.
Can you help me understand why if everyone is paying for everyone's healthcare in a socialize system - how that reforms the transparency and stops the abuses?
Because, then the single payer, can say "your policies/prices don't work with our system", fix it, or we won't cover any patients, effectively shutting you down.
What is stopping insurance companies from doing that now? If you're paying for insurance, it's in your insurance company's best interest to pay low prices.
Because insurance companies are fighting at both ends. If their payments are too low, their network providers will stop taking that insurance plan or company and then they lose customers for lack of network reach. Also, well-intentioned overhead limit regulations to spend at least 80% of funds on care, creates a countervailing accounting pressure to increase costs so that administrative spending can be higher - flowing more money to the insurance company.
I actually agree w/ overhead limits, but you also need other efficiency metrics to keep the anti-optimization in check. Or, personally I think we should go to some form of universal healthcare and wipe out private health insurance as it's currently constituted.
They can and do, at which point the hospital or other billing party directly bills the beneficiary of care or their guardian, which is how folks that think they're financially secure end up bankrupt.
A recent episode of An Arm and a Leg podcast explains this pretty well (https://armandalegshow.com/why-health-insurance-actually-suc...). In many areas of the US, health networks are effectively local/regional monopolies and can pick and choose which insurance providers they accept. So there is effectively a "single seller" system for services that are in high demand.
The party responsible for payment (the government, in this case) can tell a billing party "I won't pay you more than ___ for that service, and if you don't like it, you can sue me" without taking on the same risk that an individual would. Lawsuits are a pretty inefficient, high-overhead way to bill out, so billing parties are incentivized to not raise accountants and auditors eyebrows.
I must admit I'm skeptical of the claim that "only government can negotiate a better price"... I think anyone that's worked on government systems knows that is not typically the case.
Why wouldn't insurers argue for better prices now?
It works in 36 out of 37 modern OECD nations, with the US paying the most, and more than double all the other nations which have the government negotiate a better price.
Even in our own VA system, their negotiated prices are lower for drugs than the Medicare part D program, barred from negotiating (and with large pieces managed by private companies).
I think your skepticism should primarily be directed to wondering if private systems can ever negotiate a fair price in healthcare products and services.
There are lots of good models which all have in common a strong gov't negotiated price control somewhere in a system driven by universal healthcare principles instead of profit and market oriented principles.
I think the US has better cancer survival rates in areas than other nations, but if that is all-around significant one would think that would reflect out in better life expectancy overall. However, the US is a huge negative outlier in life expectancy and child mortality with universal healthcare nations outperforming on those measures too.
The most recent life expectancy numbers are the hardest to interpret, the US has the only three-year-running negative life expectancy growth in the first world nations - but some argue we should separate healthcare from the suicide numbers that are a big contributors. I don't know that I agree with that as there is a fuzzy line between healthcare and social care efforts.
Life expectancy is a weird stat by which to measure healthcare outcomes. For starters, it responds rather strongly to demographics. E.g. having more males reduces life expectancy holding all else equal. There are many things like this.
Age-adjusted all-cause death rate is the better stat for measuring life-saving outcomes.
Child mortality is certainly a useful stat for its purpose, though.
WHO is the best source I know of for most things like this. I was unable to find the exact stat I was looking for, but here is e.g. data on all-cause mortality rate between ages 18 and 60:
They can and do, but as per an instance in the submitted piece, you can still encounter individual providers who never agreed to that price. Then the patient is responsible for it.
I'm getting into hand-wavey territory here, IANAprofessional in a related discipline, etc., and my personal leaning is towards socializing public services such as medicine already. So disclaimed...
I think "only (any large organization) can negotiate a better price" is a little misleading on the surface. On a macro level it should, in theory, be true, and should already be happening with private insurers; when I've looked at my own EOBs, they consistently will list a service, a coding, a billed price, an "allowed" price that is always much less than the billed price, and the amount paid (which predictably matches the "allowed" price). And yeah, when we're watching politicians pontificate, we end up having strong opinions about the total price of healthcare and its effect on the economy.
That said, does anyone _really_ make personal healthcare decisions based on the macro effect on the economy? I personally doubt it.
I posit that the vast majority of US citizens and residents wouldn't care if the annual healthcare spend changed by US$200 million, but any individual American cares A WHOLE LOT if you bill them personally for US$100,000 and their insurance doesn't cover it (or much of it).
It seems to me that a much better approach to this entire conversation is "let's drastically reduce the number of Americans forced into bankruptcy because they or their dependent got sick". My own inclination is that that'll require government intervention, because the incentives for a for-profit insurance company are to pay out as little as possible, but I'm open to anything that addresses that problem.
In most cases it's not a matter of negotiation, it's a matter of law. For many categories of goods and services it's literally illegal to charge any other customer a lower price than you charge the US government. People are in federal prison today for doing that.
You have hit the fallacy on the head. Our (U.S.) system now is a terrible mess of regulations and tax breaks that drive stupid behavior. Single payer government health care is not the only alternative to what we have now. It would not produce maximums of quality, innovation, efficiency, satisfaction, or freedom. It would provide basic care to everyone.
Insurers are both victims and beneficiaries of a system in which people are terrified to go without medical insurance, but where that medical insurance often doesn't meaningfully protect you.
The proposed alternative is to give tremendous power to an organization with less conflicted responsibilities.
The presumption that competition between doctors and hospitals will create lower prices has not come to fruition. Individuals have no leverage or ability to make meaningful choices. There is no real healthcare market as a result.
In a larger system, we get lower prices via several mechanisms:
- Preventative care replacing ER care due to universal coverage
- Larger risk pool lowers per-participant costs
- Single payer has more leverage and depth of time/knowledge to regulate/negotiate with individual hospitals
The reality of a competitive landscape, hand of market, etc, that just didn't happen.
Because it's not everyone paying for everyone's health care, it's one entity paying for everyone's health care (using funds they get from everyone).
That one entity can unilaterally refuse to do business with abusive vendors. They can negotiate for lower prices. They can notice and investigate discrepancies in pricing between similar cases. They are in a position to judge which types of care are and are not cost effective and can refuse to cover the latter.
So that explains why having an insurance company helps, but it doesn't explain why a private insurance company can't perform the same role. For that, we have to introspect a little into how insurance firms work.
An insurance company is, in essence, a mechanism for transferring funds from lucky people to unlucky ones. If your car gets totaled then, in essence, a bunch of other people with working vehicles have all volunteered to chip in a couple of bucks toward buying you a new one. The insurer is mostly facilitating the transfer and skimming just enough off in the process to cover their administrative costs.
The private insurance market works well enough for most types of property because the volunteers can't predict in advance whether they're going to be lucky or not and because there's a realistic upper bound on how much money the unlucky ones will need to be made whole. Neither of these assumptions are true for healthcare. Many people were born into pre-crashed cars, to stretch the metaphor, and at least for the foreseeable future it's not possible to decide to replace a body instead of attempting to repair it.
So we need* some non-market mechanism to incentivize or compel insurance companies to cover the already unlucky: people with pre-existing conditions. But that introduces a new problem. The lucky people are being asked to volunteer to chip in more, and at least some of them will stop volunteering. That causes the prices to go up even more, which causes a few more volunteers to leave, which causes the prices to go up again, and so on. Pretty soon there's no volunteers left to transfer funds from.
So we also need* some non-market mechanism to incentivize or compel healthy people to contribute to our insurance system. And with those two requirements (needs to cover everyone and everyone needs to contribute) we are left with a problem space that the State is really the only entity with the ability to implement a solution. It doesn't have to be socialized medicine, per se, but it does basically have to be big government of one stripe or another.
\* Yes, we do technically have the option of compelling innocent people to suffer and die from otherwise treatable diseases that they're not wealthy enough to afford to cover out of their own pocket. If you're aware of that fact and comfortable with it then okay, but please do understand that it is the societal tradeoff that we would have to make to avoid some sort of serious state involvement in provisioning medical care.
They are in a position to judge which types of care are and are not cost effective and can refuse to cover the latter.
That doesn't always work out as well as you might think. A number of years back Medicare told hospitals they'd no longer pay for UTI treatment, unless the provider could prove that the patient had the UTI when they were admitted. This made sense, because hospital-acquired UTI is a big thing.
The thing is, what hospitals had to do to defend against this was to test everybody being admitted to prove that they already had the UTI. So from Medicare's point of view they were saving, but from a broader perspective they were pushing unnecessary costs (unnecessary tests) onto providers which increased the total amount being spent on healthcare.
It doesn't always have to work out, it just has to work out in the aggregate. The bar that the existing private insurance regime has set for discouraging wasteful medical tests isn't exactly high, though.
It's also worth pointing that what you're describing is an illusion of efficiency arising from Medicare implicitly pushing costs off onto non-Medicare patients. That wouldn't be able to happen if there weren't any non-Medicare patients.
"That one entity can unilaterally refuse to do business with abusive vendors. They can negotiate for lower prices. They can notice and investigate discrepancies in pricing between similar cases. They are in a position to judge which types of care are and are not cost effective and can refuse to cover the latter."
Having worked for companies that do government contract work (DoD, in particular), this line of reasoning always makes me laugh.
For non-life-threatening ER visits an app that has your insurance info and lists the Doctor prescribed treatments with their itemized cost would be ideal to see before you consent or choose what to do. For those without smartphones, the software can also be in the hospital computers ready to give a print-out. Wouldn't presenting it beforehand drive down costs? I'd be in favor of legislation requiring up-front costs to be honored, and it's on the hospital to estimate properly and/or get additional consent for added items (or have the patient sign an additional line item waiver with a limit in exchange for some incentive for the patient such an overall discount).
The app and insurance profile should also allow you put in guidance on what is allowed if you're brought in unconscious. Some may not want to be resuscitated.
There are a few procedures where a layperson could probably make meaningful decisions. How much anesthesia do you want for a procedure: cheap but uncomfortable, or pricy and painless? Should a specialist go all out to minimize scarring, or are you fine with a mark on your arm.
But for most other things, would you actually be comfortable analyzing the risks, costs, and benefits of treatments on your own? Diagnostic tests too? You're really going to say "I hear what you're saying about a possible stroke. Still, I think the CT is overpriced--and don't even get me started on the MRI—so I'll either pay for a regular old x-ray or we can just see how this numb face/slurred speech thing plays out...."
Also, how is this going to work for malpractice? The first person who opts out of the "expensive" stuff and doesn't make a full recovery is going to raise merry hell. "I KNOW I SAID NOT TO DO IT, BUT YOU EXPLAINED IT BADLY. If only I had known..."
For any ER visit it's generally impossible to predict exactly what treatments will be needed. Minor differences in treatment can cause large price variations. And the hospital won't be able to reliably predict how much the patient has to pay without actually submitting a claim to the insurer.
That's not remotely how medicine works, but ignoring that, part of the problem is that consumers don't care about costs. Why would they? Insurance will cover it.
I think this is a problem orthogonal to private versus public healthcare. I think it is a problem relating to what health insurance is today. Pretty much all hospitals get all their indirectly from patients through insurance agencies. And this is for all services from checkups to bloodwork to scheduled surgeries to emergencies.
Since the insurance companies are the middle man, the cost structures become less directly correlated between patient behavior. Demand is inelastic, particularly because insurance smooths it out. The hopsital needs so much money, so why not inflate the price of advil over here, even though it doesn't directly correlate to their costs.
> if they don't become more transparent it's going to be forced upon them.
Semi-tinfoil-hat conspiracy incoming: I think doctors and hospitals actually want government funded medical care, and are doing some of this to speed that up. Think about it. No more dealing with 100 different insurance companies or sometimes trying to bill uninsured patients: just develop expertise in handling one single government agency, and rake in essentially as much money as you care to have.
Doesn't have to be government _paid_, just regulated. Literally saying "you can't charge more than X for service Y". It isn't unprecedented either, see taxi tariffs in some areas.
Works in this context in several European countries. Switzerland for instance has compulsory insurance schemes where the prices are regulated and the insurer cannot refuse to insure.
I'd be surprised to hear of a case where price controls work, since it would go contrary to the core tenets of micro-economics. Do you have a link where I could read your source about this?
Despite the fact that in my opinion this could be fixed by Universal Healthcare I'm left wondering: how is it legal to be billed these insane amounts of money without even getting a quote beforehand? Like just waiting in the ER is worth more than buying a first class airplane ticket and getting treated in another country.
Reminds me of this really good article. TLDR: Man tried to call a number of hospitals to find out how much childbirth is going to cost him and received no answers.
Well, in fairness to the hospitals, most of us here are software developers: how many times, early on, did somebody push you to give an "estimate" for a task that was underspecified and then try to hold you to that estimate? How many times did it happen before you learned to sidestep estimates unless you already knew everything that you needed to know beforehand?
Quite often, actually. This is why we pad our estimates.
It's inescapable, in that providing a description of the problem that is precise enough to generate a perfectly accurate estimate is very close to actually just being the solution. As you do the work, the estimated time to do the work approaches the time already spent doing it.
But a lot of customers want essentially the same thing--probably a glorified CRUD app with pretty management dashboards, and a workflow that exactly parallels the all-paper workflow first designed in 1965. If you do that sort of thing often enough, eventually you get a feel for how much it costs, even with the variation across customers.
Medicine has a great advantage over software in that decades of hyper-detailed hospital billing--set up in an effort to maximize the yield of patient cash-ectomies in the face of insurer pushback--can now be subjected to statistical analysis. All those diagnosis and billing codes can be plugged back in to the billing databases to discover the median cost for the care to treat a particular ailment. It isn't so hard to then say that I am willing to pay the median actual cost, plus an X% margin for the hospital, even if the actual cost is less, provided that the hospital also eats the difference if the cost is actually more. On average, if everyone did this, the hospital still makes enough money to stay in business.
Some diagnoses in particular, such as the one every woman on the planet is likely to get an average of 2 times during her lifetime, probably while between the ages of 16 and 50, are particularly amenable to cost averaging. If you can't quote the cost of a hospital childbirth to a patient with months of lead time, including the possibility of emergency surgery, you deserve what happens to you when every actuary can crank out an answer using a pocket calculator within 15 minutes of being asked to do so. You know how much it costs. You just don't want to say, because that takes away your leverage to charge more.
But ethically, the care provider should probably not have that leverage, because if they haggle, people can die. If you cure a disease that affects 3 people in 100000, we can talk about the size of your bonus. But if you (the hospital) are on your 3rd laparoscopic gallbladder removal in the same week, and still don't know how much it costs, I want the power to set the price taken away from you.
Realistically, how am I supposed to act in a financially responsible manner when I don't even know the order of magnitude a service will cost?
Unforeseen complications are not exclusive to the healthcare industry. Imagine if you were trying to build a house, but had no idea how much it would cost. "Realistically, no construction company will give out a price; they don't know what unexpected complications may arise."
Something needs to happen here. Either healthcare is socialized (my strong preference), or the industry needs to implement some type of price transparency.
With respect to financial responsibility, if the cost of the delivery is a concern I don't think the couple in question is financially stable enough to start a family anyway. Even if this proposed change does occur there's a good chance it actually makes the procedure in question more expensive. If we start making hospitals list prices beforehand, then they're going to have to raise the base price for an ucomplicated birth in order to subsidize those that do experience complications.
Not to mention, your analogy to construction works is a good one - but perhaps not in the way you intended. Plenty of construction projects run into complications and experience cost overruns. The only situation in which I can see hospitals giving out prices is in the same context as construction projects. Non-binding estimates that are projections based on prior assumptions, which will change if unexpected situations occur.
In fact the best analogy I've come across is with car mechanics. Fixing a person is like fixing a car. The shop can charge a set rate for labor, and will provide an invoice for parts. In that sense, price is perfect transparent. But even the best mechanics can't predict with certainty what it'll take to fix a car without seeing it first. Who knows when they'll pop open the hood expecting to do a standard operation only to find that the car is messed up way harder than was originally predicted.
> With respect to financial responsibility, if the cost of the delivery is a concern...
As the GP noted, if you don't even know the order of magnitude to expect, the cost will always be a concern. The upper bound on the price is in the trillions, after all.
> If we start making hospitals list prices beforehand, then they're going to have to raise the base price for an uncomplicated birth in order to subsidize those that do experience complications.
This function is currently performed by insurance companies; a frequent criticism is that insurance should limit itself to true emergency situations, but when any routine operation can balloon in price unexpectedly, it's not irrational to want its purchase mediated through the insurance provider.
While the exact prices may not be exposed, estimates from past customers can be found online without much difficulty. If you seriously think that a hospital charging trillions of dollars is a possibility, I don't think you're writing comments in good faith.
Prices negotiated with insurance companies are negotiated under conditions very different from an uninsured patient. For example, risk of non-payment is drastically higher among the uninsured. This had to be offset by charging a higher rate so those losses are made up on patients that do pay. If you offer to pay for medical procedures in cash and immediately then you can usually negotiate the price down to a fraction of the list cost.
> While the exact prices may not be exposed, estimates from past customers can be found online without much difficulty.
They can?
Vox's reporting over the past couple years has suggested quite the opposite—that past prices are not easy to find, and that even when they are, your price can drastically vary from someone else's even for the same service. That's why they started this "submit your emergency room bills" project.
Realistically, no airline is going to give you a price for transit to a destination. They don't know if there will be a terrorist attack or if the baggage handlers on the other end will jack up their rates.
I like the spirit of this. However, what the airline is really willing to price is "best effort to provide transit to location either beginning the time stated or as soon as convenient for them after". Fortunately, their operations are predictable enough that most customers are fine with this.
That's not quite enough scope control for all services.
A terrorist attack is an extremely low frequency event to the point is being nearly non-existent. The same cannot be said of birth complications. Baggage handler rates don't change on a dime. Labor rates do affect ticket prices, but they're drastically more predictable.
Yes, but the same logic applies: you either negotiate prices out with a network in advance, or insure against the major complications. None of that is different for a health care operation.
No. The same logic does not apply, as the two situations are drastically different. The regularity of airline costs is drastically greater than the regularity of healthcare costs. Airlines can set ticket prices upfront because they predict their expenses on a given flight with a reasonable degree of accuracy. Hospitals, subject to extreme and frequent irregularities between what patients may need, cannot. At least not with individual patients. Insurance companies are very different types of customers as compared to individuals. Because the negotiated price applies to a large group of people, the question isn't "how much do we have to charge to break even on X procedure?" The question becomes, "How much do I have to charge for X procedure, *averaged over hundreds or thousands of patients?". Each patient is effectively a slot machine for the hospital. Insurance companies negotiate on behalf of a large number of patients so that the aggregate cost becomes something that is predictable enough to negotiate.
My veterinarian manages to give quotes - before they do emergency treatment, they come up with a low, typical, and high quote, and I have to agree to pay up to the "high" price before they'll start the treatment (if I refuse, then they'll come up with an alternate, possibly less effective, treatment plan.
It's a little harder to do that with humans since they aren't going to pause an operation, keep the incision open, and tell the spouse "We found an unexpected tumor, so let's wait an hour while we generate a new quote and you can decide if you want to pay it".
But that should be part of the quote "Unexpected events can cause us to exceed the quote", and then they should have to document why it was unexpected.
They have nice pricing tables for insurances,. Just not for patients. Even unexpected complications will have a billing code but the prices are kept secret.
Insurance companies are very different types of customers than uninsured patients. They're effectively averaging their price over a large number of patients. Most are probably slightly more expensive than necessary, but that difference helps subsidize those that experience complications. Furthermore, individual patients fail to pay at a much higher rate so that is reflected in the cost as well. A hospital can't just give the "insurance price" to uninsured patients as this may put them underwater.
Try a private hospital in London[1] — it's £7,585. This is presumably high-end; it's a place princesses and sheiks' wives go to give birth.
It says "Additional charges are made if you require critical care. If your baby requires transitional or specialist care, this is free if they are entitled to NHS care and is chargeable if they are not."
But the hospital doesn't know if the birth is going to be uncomplicated until it actually happens. If the hospital gives out only a projected price, then it could lure people into false sense of security. A non binding price is effectively ad worthless a no price.
> But the hospital doesn't know if the birth is going to be uncomplicated until it actually happens. If the hospital gives out only a projected price...
The hospital can totally give a realistic, projected price: It can know what the probability of a complicated birth will be, and it is also able to amortize that over all the uncomplicated births.
There's no sane public-policy reason it should be structured like a reverse slot machine: you pull the lever, get a fixed prize, then find out how much you'll pay for it.
If it's a projected price, then the original commenter is still screwed if the birth becomes complicated. It's still a slot machine. Furthermore, it would incentivize sketchy practices like setting a lower base price than competitors but aggressively discovering (or manufacturing) complications so that the average price is considerably higher than the base price.
Not necessarily, it could be the hospital that gets screwed, they can eat the extra cost of the complications -- that could be factored into the base price, add X% to the bill account for the slight possibility of an unexpected complication.
Health care is the only industry where the felony laws regarding up front pricing aren't enforced. It was allowed to become a twisted regulatory nightmare where the laws were written by the industry itself utilizing kneejerk methods to obtain profit at the cost of systemic corruption.
It takes a while to realize nearly every law is anti-competition protectionism. I didn't realize it until I was working for a multinational food company and the managers were bragging about how the company lobbied for a safety bill that exactly regulated their own industry in a way that cost their competitors billions in compliance fees. They were proud of it. I was disgusted.
Disgusting, but know that there are good regulations—like environmental protections—that are frequently combatted by industry groups and tend to get weakened by the Republicans before they pass into law. Regulation can be abused by industry and corrupt politicians for anticompetitive reasons, but most of the time, it's to force companies from doing highly profitable things that aren't good for people or the planet; its much cheaper to just dump all your hazardous waste into the river, after all.
"Regulation" is not a monolith, the specific details of a particular regulation are absolutely essential to evaluating its efficacy. This tendency to suggest that all regulations are bad reflects an ignorant perspective.
This is a non-sequitur. For something like emergency care, where the choice can literally be "pay up or die", a private provider has every incentive/opportunity to charge outrageous fees. Because what are you going to do? Tell the heart attack to wait while you find another provider?
The price-opacity may be a product of regulation, but the prices themselves are free market capitalism working as intended. For another example of the same, consider the recent reporting on collusion between generic drug companies[1]. When you can't refuse to buy the product, the vendor has a ton of power to set prices as they wish.
"The prices are high — even for things you can buy in a drugstore"
Reminds me of the brief hospital visit I had in Paraguay where I needed to have a friend or relative always with me because the hospital didn't stock anything. If ibuprofen, bandages, syringes, antibiotics, etc were needed, the hospital staff would tell me and I would have my friend or relative run across the street to buy the necessary supplies from one of the pharmacies so the doctor or nurse could treat me.
Cheap hospital bill, cheap pharmacy bill, pain in the butt for my friends and relatives.
I know $60 Ibuprofen can seem like a lot, but is anyone arguing that you're literally paying for only the pill(s) with that $60? Aren't you paying for the instant availability, the insurance that it's not expired (do they even expire? I really don't know), and confidence that your healthcare provider has signed off that XXX mg of Ibuprofen is a.) OK to have with your current medications and conditions and b.) sufficient to do the job? Isn't some of that cost the healthcare provider's expertise and service? Would it be better if they prescribed morphine and charged you a magnitude more when ibuprofen would have done the job?
I charge clients similarly. I overbid projects that I don't really want to do. If you want me to setup Wordpress for you, I'll charge you out the nose. Granted, you get to accept my fees before I ever send you a bill. It's not a perfect analogy.
> This is all due to the key fee I’ve been investigating this year: the ER facility fee. This is the fee that ERs charge for walking in the door and seeking care, something akin to a cover charge at a bar.
This seems absolutely reasonable to me, I wish I could charge a 'fill my email with RFPs' type fees. Walking into a waiting room, signing in and waiting is not nothing. You and your symptoms get evaluated and triaged. That takes expertise and know-how. The prices vary wildly because different hospitals experience different levels of demand, I imagine.
> I know $60 Ibuprofen can seem like a lot, but is anyone arguing that you're literally paying for only the pill(s) with that $60? Aren't you paying for the instant availability, the insurance that it's not expired (do they even expire? I really don't know), and confidence that your healthcare provider has signed off that XXX mg of Ibuprofen is a.) OK to have with your current medications and conditions and b.) sufficient to do the job? Isn't some of that cost the healthcare provider's expertise and service? Would it be better if they prescribed morphine and charged you a magnitude more when ibuprofen would have done the job?
It's hard to argue the 600x markup is there to cover overhead when they literally have a facility charge there to cover overhead.
You also have separate line items for each of the things you mentioned -- doctors, nurses, staff, etc. You are paying for that expertise, often many times over, in addition to a $60 pill that retails for $0.10 at the local Walgreens (who also manages to make sure that it's not expired).
Absurdities like $60 Ibuprofen seem like an unforced error to me. This is the kind of blatant abuse that leads to voters getting collectively angry and getting the legislature involved.
You also have to cover uncompensated care, which is a significant chunk of change at any hospital in a major metro area. Besides, nobody actually pays the charges. Insurance companies don't, CMS doesn't, and even the uninsured can typically negotiate a bill down with a quick phone call. That's why the charges are all made up bullshit. It doesn't matter so why bother?
Most hospitals in the US are non-profits. You can go look at their financial statements yourself. They're not exactly raking in the dough. Running a hospital is enormously expensive, and if somebody comes in needing $1 million worth of care, then you're required by law to give it even if they can't pay.
That money has to come from somewhere. That's why Ibuprofen is $60.
I'm guessing you tell your clients, "I'm not really the right person to set up WordPress for you. I can do it, but it'll be incredibly expensive. You can probably do it yourself with a good online tutorial."
Hospitals aren't telling their patients, "We're not really the right institution to give you ibuprofen. We can do it if you really want us to, but it'll be incredibly expensive. You can just go buy some at the store for like ten cents." In fact, I bet that even if you have the presence of mind to decline their ibuprofen because you'd rather get your own, they'll strenuously argue against it, or even start treating you as not following medical orders.
In any case, it would be a lot more palatable if they'd charge marginal costs for marginal items, and charge overhead separately. It may well cost them something on the order of $60 to give someone ibuprofen, on average, but it does not cost them $60 more to give one more person ibuprofen. It would be more honest to charge two cents for the pill, and separately charge your fair share of the cost of the staff that obtains, vets, distributes, and administers that pill along with everything else you're getting.
I think the difference just having a hospital triage you and tell you 'ibuprofen will handle the pain, it's nothing serious' is _already_ worth a boat load of money and peace of mind.
I agree with you - it would be really interesting to see honest and transparent itemized bills, with separate items for overhead. I wonder if people would have the same problem with high bills in that case. Probably wouldn't like the total any more, but maybe it'd be easier to understand.
That’s definitely worth a lot. But the difference in price between “you just need ibuprofen, pick some up on your way home” and “you just need ibuprofen, so take this pill” should be minimal.
My understanding is that the $60 ibuprofen was a line item amongst other charges. Everything else you mentioned is likely covered by another line item in their bill. It's not as if they went to the ER and got a bill of $60. They perhaps got a bill of $500, of which the breakdown mentioned $60 for ibuprofen.
It's kind of like going to a mechanic and getting a bill of $200 for a single headlamp bulb, and another $300 for labor. Then the mechanic arguing that the $200 for the bulb includes the mechanic's expertise, knowing which bulb to buy, etc. Umm...no. All that is included in labor costs.
>This seems absolutely reasonable to me, I wish I could charge a 'fill my email with RFPs' type fees.
Do you not think that fee should encompass doctor's expertise, instead of sprinkling that over cost of materials?
My initial reaction when I read the piece was in agreement. I think it makes sense for ERs to have a facility fee. However, it doesn't explain how one hospital's facility fee can be, say, double that of another. Is it that one hospital is using Hue lightbulbs compared to the other?
A $5751 bill which is almost entirely a facility fee is ridiculous.
I would imagine a facility fee should be relatively fixed - it is the cost to maintain the facility and has nothing to do with a given patient's medical condition. As such, it is trivial for a hospital to publicize the fee and provide transparency.
In general, I think all the items they bill for are reasonable. The amounts, though? Not at all. When you start looking at the variation in how much is charged for the same items across different hospitals (or even within), there is no good model that can provide an explanation.
If they told me it would cost $60 for a simple Ibuprofen, I'd get out of bed and walk myself down the pharmacy on the first floor where they are regularly priced (in the SAME building), or send a family member down for that 10 minute walk to save $50 times how many you need to take. The pharmacists know the drugs I'm taking and interactions, yet the Ibuprofen isn't marked up a couple hundred percent.
While my wife was recovering from surgery in Nevada, the surgeon literally said “I can have the hospital give her these pills I’m prescribing her (OxyContin or something similar), but it will cost you a lot less to get them from the pharmacy across the street and give them to her when you go home.”
I don't think this argument fully makes sense, because there are already separate charges for the services you describe. The physician who sees you will send you a bill, as will the facility.
> I charge clients similarly. I overbid projects that I don't really want to do. If you want me to setup Wordpress for you, I'll charge you out the nose. Granted, you get to accept my fees before I ever send you a bill. It's not a perfect analogy.
A more apt analogy might be you installing a Wordpress plugin that costs $10 for a client, then sending them a bill that looks like this:
$1,000 - Install fee
$1,000 - Plugin license
=========
$2,000 - Total
Then, when the client complains that you sold them a $10 plugin for $1,000, you say "Yeah, well, you weren't just paying for the plugin, you were paying for my time to install it" even though you had an additional charge for the time you spent installing it.
I don't think I have an issue with $60 Ibuprofen (or one thing being upcharged), it's everything being so upcharged, with the expectation that it's going to be negotiated down by an insurance company, and then if you don't have insurance, they try to get you to (or at least pretend) that they haven't overinflated everything and you owe them every penny, unless you just don't pay them, and only then will they consider accepting less.
The law doesn’t require you to serve your customers regardless of their abality to pay. You don’t have a set of customers who have figured that out and come to you for services outside your core competencies.
The market also doesn’t expect you to accept payment terms much worse than NET30.
And a hundred other ways that healthcare is a tricky business. If we want to fix price transparency, we need to fix all that too.
> Isn't some of that cost the healthcare provider's expertise and service?
In theory maybe. Usually I would say these things are not exactly top priority and you are not getting your money's worth in the premium there. At best, of your list, you're paying for the instant availability, but what about the times where it's not instantly available? You're not paying for a guarantee of it.
In the UK patients pay a flat charge for a prescription which is around £10. For that reason I rarely prescribe something like ibuprofen or paracetamol outside of the hospital. I will always tell the patients to buy it themselves over the counter for around £0.16, unless there is a good reason to deliver it via a prescription.
Insurance companies generally get “most favored nation” clauses so that they all pay the same price as each other. EOBs show the list price for a service, and the much smaller amount actually paid. The people who really get the short end of the stick are uninsured: they only see the list price and maybe an offer to negotiate.
> I charge clients similarly. I overbid projects that I don't really want to do. If you want me to setup Wordpress for you, I'll charge you out the nose. Granted, you get to accept my fees before I ever send you a bill. It's not a perfect analogy.
One can always forgo setting up WordPress, which is not always the case with healthcare.
Great article. I think the narrative around health care is often around who has access to good insurance and who doesn't, and as the cost has skyrocketed we have doubled down on that debate. The real problem is that health care providers won't or even can't tell you how much something costs. This has set up this situation where, since money is not part of the decision making process, they just keep raising costs. Imagine a grocery store where prices are not labelled, and you get a complex bill a month afterwards. And every grocery store does this. What are the chances prices for groceries are going to be competitive? Zero.
If we can find a way to bring market forces to bear, it will pressure healthcare organizations to reorganize themselves to provide services in a more affordable way. And before anyone gets sanctimonious about putting money over quality care, consider the actual harmful effects of these crazy bills on people's lives. I used to do title work, and I became familiar with a pattern of people quietly paying their mortgage on their house for a couple decades, no liens, and then all of a sudden a lien from a hospital bill shows up. And then everything starts to crumble, other liens accrue, and I'm doing the title search for the foreclosure. A family just got moved from middle class to living in poverty. Our healthcare system is becoming a vehicle to impoverish people.
> If we can find a way to bring market forces to bear
I think the problem (also outlined in other comments) is that there are no market forces in the US health services market. There is no pressure to provide less expensive services, no pressure to reorganize, and no reason not to do what is being done now: build a non-transparent system where people get charged arbitrary amounts and prices are not known beforehand.
Let's be careful to not look at one type of health care, emergency care, and generalize to all types of health care. Right now we all (Americans at least) don't really have insurance. We are part of pre-paid health clubs and we try to use the health club membership to pay for everything. For true time-sensitive emergencies we should all have traditional insurance, and yes, the services should probably be supplied, like fire fighting, by non-profit organizations.
Health care that is not time critical should not work like the fire department. In fact, emergency rooms, once they diagnose something as not being an emergency should be able to say, "sorry, this isn't the right place for this, go to a doctors office."
With non-emergency care we should all be able to get price quotes up front, we should be completely aware of our choices and the be able to shop around. We could maybe outsource that to health care clubs like Aetna and UHC if we choose to (knowing that we are getting less choice and that we'll have to deal with those bureaucracies as a trade-off), but there shouldn't be any tax breaks or employee incentives for using those health clubs.
I recently had surgery to have my vision corrected with no "insurance" (or health care club) involved and it was so nice. I shopped around, the doctors all competed for my business and treated me like royalty, there was absolutely no confusion over price, there were financing options available, the technology was cutting edge (or I could have chosen to go less cutting edge and paid less), it was incredibly refreshing. I'd love if most of my health care could be like that.
This works reasonably well for things like vision care because they're entirely opt-in. Patients who aren't satisfied with the prices they're being quoted can realistically choose to keep wearing glasses instead.
No one in their right mind is going to decide that the going rate for chemotherapy is a little steep right now so they're going to sit with the cancer for a year or two and see if the prices come down.
A) We do have socialized food insurance. That's literally what EBT is.
B) I'm not going to wake up in the morning to discover that my expected annual food costs have suddenly increased by four or five orders of magnitude. There is no budget-conscious version of a lot of non-emergency, but still lifesaving, medical care.
A) Right. We have universal single payer food insurance, also known as taxpayer funded welfare for the poor. We're in essence covered by, and paying premiums to, a mandatory State-run insurance policy such that if we ever can't afford the minimum necessary food to survive the State will (at least in theory) step in and buy it for us from the open market.
B) Let me rephrase. I'm not going to wake up one day to find that my required daily calorie intake has increased by multiple orders of magnitude. There are very few household budgets that could reasonably be expected to absorb such a shock, no matter how efficiently the market for those calories functions.
A) and it works like insurance in that most of us don't ever need it, but it's there just in case. Also, it does not regulate prices, providers, etc.
B) Again, yes, we need health insurance for rare surprises just like we get fire insurance, auto collision insurance, etc. in case of those rare occurrences. We do not need insurance for medical treatments that everyone gets. We just need to plan ahead financially for those, just like we do for food, clothing, housing, etc. Preparing ahead of time for known expenses is not insurance. If everyone's house burned down a few times each year fire insurance would not work, you would instead just factor that in to the cost of living.
As I understand it, we have a relatively small number of people with serious or chronic illnesses whose normal, predictable healthcare expenses will drastically and permanently outstrip their realistic ability to pay. The only way they will ever be able to receive treatment is on someone else's dime, one way or another. And because everyone involved knows they're going to cost more to treat than they can pay then no sane insurer will willingly cover them if they have a choice in the matter.
As far as I can tell the main difference between the socialized food insurance we already have and the socialized medical insurance I'd like us to have is that subsistence level food costs are uniformly low for everyone whereas subsistence level medical costs vary wildly from person to person.
Vision and dental are areas where the market is halfways working. If you get a planned surgery the hospital will still try to rip you off left and right. It's not only emergency.
Last year my 1 year old baby had an accident in Germany. She fell off of a bed. I took her to an ER and after the examination I paid approx. 100€ = ~100usd. I assume in USA I would have paid 10kUSD or more..
$10K? That's ridiculous, I really wouldn't expect any kind of trauma visit to be that cheap, the ambulance ride alone could be over $2000 and the hospital could charge a "trauma activation" fee of $5,000 - $15,000 which doesn't include any treatment at all, that's just the price to have access to the ER facilities.
I wonder what healthcare bills would look like if they were itemized so that things like Ibuprofen were literally billed at cost ($0.25 per?) and there were line items for services/labor that captured the real cost of being a medical professional:
- Emergency room wait: $0.10 for lights
- OTC eyedrops (4 drops): $0.20
- Triage by on-duty nurse: $100 (@ $300/hr)
- Consult by on-duty physician: $220 (@ $600/hr)
- Late-night convenience fee: $100 (between 7pm and 7am)
etc. I made up all the numbers, I have no idea how healthcare professionals calculate their hourly rate.
IIUC, much of healthcare billing in the US is governed by discrete codes for services performed. I suspect this allows big customers like Federal Gov't & insurers to audit bills easier. In order to either be more specific about the bills or allow less wiggle room, they made these codes remarkably more specific recently (ICD-10 [1]). IMO the descriptions of the items in these codes are humorously specific. Imagine if your auto mechanic got $650/hr for labor, I suppose you would get much more specific invoices for their work too.
Many ER bills are broken down similar to that now. I was in the ER earlier this year for about 12 hours and there were 30 different line items. The big ones were "part trauma tm response activat" for $26k, "critical care 30-74 min with mo" $5.5k, and a couple related to ct scans. I was only billed $5.92 for ibuprofen 600mg.
I'm surprised to see lots of people in the comments talking about line items. Line Items are irrelevant. They could include line items for oxygen and toilet paper if they wanted to. The hospital charges whatever the market (and where applicable, regulations) allow. The configuration of the line item is pretty much a customer service problem: 'how do we show what we've done in a way that will get the customer to pay it.'
> The hospital charges whatever the market [...] will allow.
Except that in this case, the market is paying before being told the cost. So, what is enforcing the upper limit on price in this type of bizarro market?
There is an issue with what I'll call the "consumer-market" theory in emergency healthcare in that there is no transparency in pricing at time of purchase or prior to purchase.
How can markets function without price-transparency?
It makes me sad that there are places in the world where people have to pay to go to an emergency doctor. I know it’s a political hot topic but all that aside doesn’t most people deep down inside think that every fellow human should have the right to free doctor?
Okay, sure, I agree in general, but how far do we go with this?
Does every other human have the right to extraordinarily expensive, often unproven cancer treatments only available at research institutions in the United States? Are we willing to start making cost based decisions on who should die (i.e. should we really be spending hundreds of thousands of dollars keeping those above 90 alive for age related illnesses?)
Everyone will want everything free, but for this to work you have to make uncomfortable decisions. If you put nothing into the system, how much should you get out? Should others with more resources then be able to then buy private insurance for access to better care even though that sounds "unfair"?
Everyone always glosses over these fun questions when they talk about universal health-care systems.
Those are red herrings. Many (if not most) countries somehow figured it out without having to deal with absolutes and black/white decisions. You can (and should) draw a line somewhere, and this can be done reasonably.
As a European living in the US I find it mind-boggling that the richest country in the world does not consider universal healthcare to be a fundamental right of its citizens.
1. Your first point about "unproven cancer treatment" has an overly narrow focus on the edge of medical research. These cases are yes something that needs to be addressed, but they are far from the norm of normal medical care.
2. I've never heard anyone ask for anything free related to healthcare. There is very little truly free care in the US. The conversation here is about price transparency and what is considered reasonable.
Absolutely not. Just look through this thread. So many people fetishize "markets" to the point where they act like it's reasonable for people to simply roll over and die if they haven't achieved a certain level of wealth, it's disgusting.
I'm patiently waiting to have injuries and sudden symptoms until ER bills become more reasonable and transparent. Until then, if something happens, I guess I'll just die.
This is outrageous because the regulation wouldn't even have to be complicated. In the EU there is a directive that you have the rights to know the retail prices of things before you make a purchase and in some countries, retailers have to honor the lowest posted price and we are talking about baguettes!
I don't see why that same thing couldn't apply for healthcare.
1. ERs should publish prices in a public database. If a price is not published for an item/procedure, the customer can pay the lowest price she/he can find for the same procedure from an other provider.
2. The same price must be charged from everyone (regardless of insurance).
Even if only a small fraction of people shop around it might push down the prices. Even if the above is too naive, I am sure someone smarter can come up with a less naive version of it.
"1. ERs should publish prices in a public database. If a price is not published for an item/procedure, the customer can pay the lowest price she/he can find for the same procedure from an other provider. 2. The same price must be charged from everyone (regardless of insurance)."
+1. Moved from UK to Australia and it is very similar here too in that most medical care is free.
One difference is that the ambulance service charges for residents, and usually it is reasonable priced (but not cheap) but if it turns out you need a helicopter the bill can be quite large! But insurance covers it. For most professionals insurance is very cheap because of the tax saving you get.
It's fantastic here too. I had a scare recently and called the ambulance, was at the hospital pretty quickly, got an x-ray, stayed overnight, turned out not to be a serious thing but finally figured out what was causing it. No drama and no crazy $100,000 bills. Just healthcare of an acceptable quality when you need it.
There is just no way that any perceived marginal improvement in the quality of care on an individual basis warrants an off chance of maybe being bankrupted. I can't say I've ever found the quality of care of be poor or unacceptable. It's always been available and served me well.
I kind of liken it to being forced to drive an $80,000 BMW as opposed to being provided with a reasonable Toyota that does the job.
The economic experiment has been tried and the US is on the wrong side of it.
I've sadly been to hospital via ambulance quite a lot for seizure activity and that kinda carrying on. The biggest bill was when I received my $54 bill for the ambulance! Oh no. (St John is a volunteer ambulance service). So, I went and paid it and then paid them $80 for an annual househould membership - meaning if anyone in my house ever needs an ambulance, it's free!
I'm aware however, with the rescue helicopters there can sometimes be complications because at the end of the day, someone needs to pay - but as an accident, everything's covered under ACC anyways. (and: http://www.police.govt.nz/faq/if-i-get-lost-and-need-search-...)
Wow, the more i read, the more difficult it is for me to believe. At this point i feel that the US healthcare industry is the biggest rent extraction industry in the world and they try to get away with it to the extent they can with every stakeholder blaming someone else.
I have lived here for 9 years and although have paid my insurance diligently i always get anxiety at going to the doctor's office.
Pretty much the same as Aus and UK, though I think some level of subsidised healthcare for visitors though surgery, etc. will be charged in full, and full coverage for permanent residents, where as Aus tends to charge full price for everything, I believe (still cheap compared to the states though).
Doctors (GP) visit typically costs me around $40-50NZD, thats likely on the high side, Children are free / fully subsidised.
A&E visit would be $50-100NZD
Most all injury related medical costs are covered or subsidised by ACC.
Specialists Appts typically cost ~$200 per visit
Private health insurance, while in no way "required", is still offered by the bigger employers and will see better outcomes for elective and non-urgent surgery and is priced in the hundreds of dollars per year for "basic" coverage if you wish to purchase as an individual.
> I started my project focused on one specific charge: the facility fee. I found this charge for walking through an emergency room’s doors could be as low as $533 or well over $3,000, depending on which hospital a patient visited and how severe her case was. I also learned that the price of this charge had skyrocketed in recent years, increasing much faster than other medical prices for no clear reason.
Is this why my local hospitals are advertising their ER wait times? The arbitrary profit from arbitrary "in the door" fees?
I'm curious what percentage of costs were covered by insurance. I recently had some genetic testing done and they were pretty open that they charge one lower price if I paid out of pocket and another higher price if insurance covered it. My hunch is that some of the price variation is just from providers magically increasing prices to match whatever the insurer is willing to pay.
>3) You can be charged just for sitting in a waiting room
I once fainted during a comedy show because the comedian was talking about his wife almost dying in surgery in graphic detail and I got nauseous and fainted. I woke up outside the comedy club up against a wall with an ambulance there. They basically took my blood pressure and gave me a bottle of water then asked if I wanted to go to the hospital. I declined. I still received a $3000 emergency services bill later... Apparently they checked my ID/insurance when I passed out and somehow I ended up with a bill even though I declined service.
In contrast, I once hit my head on a train in France and had a huge gash that needed stitches. I took a taxi to an ER, got seen within 20 minutes, left the ER within 90 minutes, then had a $50 Euro bill.
The contrast between "socialized" healthcare in Europe vs privatized healthcare in the US is shocking. We receive far, far, far worse quality and fewer services despite paying a lot more. We're in the worst of all situations.
I don't see the situation changing in the US anytime soon. In order for us to have single-payer healthcare, doctors would need to accept drastic pay cuts, pharma companies would get far less for drugs, and insurance companies would go out of business. None of that will happen. Instead we'll have more and more and more regulation until it just stops working.
I'm not saying the ER prices are reasonable, but an ER has to keep a lot of expensive staff and equipment sitting around until they are needed. OK, some ER's they are sitting around. But there is a price to have all that service ready for an emergency.
As for high drug prices like the $60 ibuprofen, you are mainly paying for it to be delivered to you by a nurse.
ER's have an average profitability of 7.8%. Higher than Walmart but lower than Apple. So if they became non-profit in some way, they could cut that percentage of costs. That's some, but still very expensive.
The thing is the "paying for it to be delivered by a nurse" is covered by other things.
There will be a line-item for the ibuprofen itself, there will then (generally) be a separate line item for staff time spent helping you, and there will almost always be another line item for the facility fee.
The nurse's overhead is theoretically included in those latter two line items, so shouldn't _also_ be charged in the ibuprofen line item.
Now, there are logistical concerns that will make the ibuprofen marginally more expensive at an ER than at a clinic, but definitely not $60.
I accept the logic of high drug prices including staffing costs when those staffings costs aren't included in other line items. In most hospital bills, it seems, those staffing costs are already included.
Reading this article and seeing all the startups sprouting in the field of health care and medicine tells me that there's still a lot more areas to innovate and disrupt in this industry.
One big issue though are that lobbyists who wanted to keep prices high - to squeeze in as much profit as they can out of these. Drugs, Antibiotics, Procedures, Medical Professionals. I know it would be far-fetched to standardize and at least provide some level of transparency across all facets of operation in this field, but that would be a good start.
Analyze the data, and find ways where things can be improved incrementally.
One way to disrupt the industry might be to have everyone be in one giant insurance pool, perhaps paid for via taxes, and then give everyone access to health care via some kind of non-profit entity.
Sounds crazy, right?
It worked well for my family and I during the many years I spent in Italy, which has health care costs that are something like half of what they are in the US in terms of GDP.
Yup, it's worked nearly all over the modern world, for years and years. The last thing I want in healthcare is more startup maniacs trying to "disrupt and innovate" when there is a clearly viable alternative.
All this value being captured by middlemen “sprouting” up could also simply mean more money out of the pockets of healthcare customers, who already are going bankrupt paying for all of this inefficiency. The US healthcare industry is a raging river of money coming directly out of the wallets of consumers who have little choice. Not surprising that it attracts middlemen with spoons ready to dip into the river.
How are you going to get it? Even Google has huge regulatory issues around touching health care data. Medical records are some of the most highly regulated pieces of information around. A startup would have to have very deep pockets (or a few lawyers as founders) to have any chance IMO.
I'm in the industry right now, and while there's certainly room for innovation and improvement (our company was one of those originally), anyone considering it should know that this industry is a huge legal and regulatory quagmire, which makes diving into it difficult if you're not already familiar with it.
Despite knowing a lot about how it works after being in the industry for several years, I don't think I'd have the stomach to take a stab at a startup in this field myself. I've already had to deal with it over the years as an systems engineer and I'm pretty sick of it.
Also, if you're planning to do business with the big companies in this field, at least from the standpoint of my company, they really drag their feet with signing any business deals with you, and just about every company doesn't really want to pay you to do anything. We've had multiple companies back out of contracts (or act like they're going to sign once things are negotiated, then don't), even after we've done significant development (in one case building a whole system for them) and not pay us for our work, and then have the gall to ask us for parts of the code afterwards.
The only reason we did that work also, is because there are some crazy hard deadlines with open enrollment and the process drags so much that by the time everything is signed the software basically already has to be complete immediately upon signing if we wanted their business or else it would miss the open enrollment window (or pre-open enrollment, or whatever else hard deadline they had).
Also, the industry has been upended and thrown into chaos with Obamacare, and if the Republicans ever succeed in repealing/replacing it, then it will probably be thrown into chaos again. This creates an opportunity for startups that can move much quicker than these behemoth companies can move in reaction to these things, but it also means that you could be building a business on top of quicksand, and might have to make significant and expensive changes yourself in a few years if it changes underneath your feet as well.
Florida typically comes dead-last consumer protection-wise except that it requires ER physicians to be "in-network" when the hospital is also "in-network".
I often find in these discussions that Americans look with undue admiration over to Europe and imagine that the same stuff doesn't happen here.
But it does.
I recently got my wisdom teeth pulled out in Germany, and without my asking, the doctor sent me a pack of 12 Ibuprofen and billed me 24 euro, i.e. €2/pill. I didn't want them because I had 500 of the same at home, which I bought for 25 euro — i.e. €0.05/pill. That's a markup of 40x.
There is a documentary on HBO now called Bleed Out. If you want to know how absolutely fucked the US medical system is, watch it. You will probably never want you or anyone you love to ever step foot in a hospital again.
These insurance companies and hospital groups are pure evil. Absolutely disgusted with what a backwards ass country America is.
This "ED is too expensive" situation has been going on for decades.
Is it possible the fairly new walk-in clinics could help?
Could there be a big red sign on the ED door saying, "Hey we are very expensive and if your condition isn't serious you will wait a long time! Consider using the walk-in clinic at 123 Main Street."
I stopped reading when I saw the minimum charge for walking through the door was USD 500 and that a family was charged USD 18 k for a nap and some formula milk; it was just too depressing.
No amount of analysis of the details is going to fix those things.
It would be interesting to compare prices with countries with free government sponsored medical care. In NZ I know they work out the cost, and if you aren't a resident/citizen you have to pay the bill.
Is NZ healthcare decent? Asking because i am trying to decide between NZ and Canada as my future destination for immigration after living in US for 10 years.
Meanwhile in Russia: free ER services, free nationwide health care and no-franchise cheap voluntary insurance for everyone who doesn't want state medicine.
Cheap because you have to compete with rather-good and completely free for everyone.
Like literally, have some government body write a table:
1 pill of 400 mg paracetamol ............ $0.50
1 pill of 800 mg paracetamol ............ $0.60
prescribing medicine (once per day) ..... $4.32
base fee for an ER visit .............. $200.00
5 minutes of work by an ER physician ... $27.43
etc. and impose that as the maximum price that can be charged.
It's not going to happen because "omg socialism", but this is literally how other countries handle it. Possibly with a multiplier that the hospital/doctor can apply within certain limits. If you really need to, maybe even allow deviating from it as long as the patient is conscious, in a position to make that choice (i.e. not emergency care), is explicitly informed that this is above the "official" rate, is informed about the rate, and signs off on it beforehand.
And I'd like to point out that this sort of regulation isn't unprecedented in the US either. Taxi prices are regulated this way in many areas. Apparently, transportation is more important and less suitable to be left to a free market than healthcare...
Shouldn't the max price of services (not things like RX of course) be different depending on the cost of living in that area? You'd need different prices in different areas otherwise the prices might be too expensive in some areas and too cheap in others. If the prices set are too cheap, you might see more people using the ER for non-emergency purposes, which would be bad for the people that need to use the ER for actual emergencies.
> If the prices set are too cheap, you might see more people using the ER for non-emergency purposes, which would be bad for the people that need to use the ER for actual emergencies.
The "long wait times" that Canadians sometimes complain about actually address this problem within public healthcare. If you come into the ER for a non-emergency, fine, but prepare to wait 4-6 hours. Every emergency case coming in the door will get placement ahead of you.
Some provinces (e.g. Ontario) address this with phone triage hotlines that help you make a decision about whether to go to the ER, a walk-in clinic, or wait for a doctor's appointment.
Universal-Care citizen here. Let me explain how it works. It's definitively not "first in, first served": when you reach the place, you get "pre-examined" by a doctor, who estimates the urgency of your case. Fast, like, in minutes. He assigns you an "urgency level". You then have to wait more or less depending on that. I don't know the exact algorithm they use, but I would assume it's some kind of weighted queue. If you go to ER with a headache, you will have to wait for a long time.
This probably helps but is not the sole solution. The state of Maryland has done this for 40 years and they have some of the highest Medicare hospital prices in the country. The problem seems to be consolidation: Johns Hopkins has gobbled up most of the other hospitals in the state, and so has significant control over prices.
(Source: my wife worked at a rural hospital on the border in a neighboring state.)
The idea suggests itself that the problems of the US healthcare system are closely tied to unrestrained capitalism, includings its influence on/over US politics.
A question that frequently comes up in healthcare debates is "would you rather be alive now or alive with the medical technology of 1970".
You'd be giving up genetic testing, numerous advances in wound care, a number of advanced antibiotics, leaps in transplant technology, and a whole slew of joint-replacement innovations. Plus cancer treatments, and of course, AIDS therapies. Massive impacts, right?
And if today is better than 1970, 1970 was better than 1950, and 1950 better than 1920, and....
Right?
Not so fast.
New York City have been tracking mortality rates since 1800, and there's a chart I love to pass around in these discussions, with the charming cocktail-party friendly title of "The Conquest of Pestilence in New York City ... as shown by the death rate as recorded in the official records of the Department of Health and Mental Hygiene".
The 20th century has seen a host of medical advances: antibiotics, vaccines, transplants, tailored drugs, implants. High-cost, yes, but huge impacts.
The turning point in the chart -- where the increase in mortality as New York as it grew from a town of 60,515 (1800) to a city of 813,669 (1860), was the formation of the Department of Public Health itself, in 1866. Peak mortality hit 50/1,000 in the 1830s, 180s, and 1860s, with a sustained average above 35/1,000, and marked volatility as the city was rocked by epidemics. By the 1890s, it had fallen to 20, and 1920, about 12. The pre-WWII low was actually in 1939-40, at just over 10, and mortality rose through the early 1970s. There has been a further decline, to about 7.5, since 1990.
Analysis elsewhere suggests that this is almost wholly attributable to increased longevity among minority populations -- nonwhites generally, black women, and especially black men. My suspicion (though I've not researched in depth) is that this is largely attributable to increased access to medical care, either through improved socioeconomic status and access to the commercial healthcare market, or through public health programmes. There is little if any evidence that the gains come from medical technology itself.
This is a topic that's been much studied. Robert J. Gordon's epic assessment of US economic progress, The Rise and Fall of American Growth (2016) looks hard at medical advances, particularly since 1970, and finds them largely absent. Victor Fuchs, healthcare economist (heavily cited by Gordon) has found published similar results for the past few decades.
A personal anecdote is a close friend who'd died of an obscure cancer in the early 1990s. The (brutal) treatments they'd undergone were essentially unchanged since the early 1970s, or even 1960s, as I read the literature, and have changed little in the ensuing nearly three decades. Given that one of the questions and agonies we faced at the time was "what if some miracle cure emerges, or we weren't doing enough", this failure-to-advance is in some ways a bit of validation: we really try to do everything we could, and applied the best available knowledge, and no, even now, the outcome is virtually unchanged: four out of five patients with that diagnosis die within five years, often less.
(Other friends have survived their, mostly other, cancer diagnoses. And of the cancer-friends we'd made, some are still alive, others have died, in cases of complications from treatment, including blood- and tissue-donation related infections such as hepatitis. Life is not fair.)
Real healthcare improvement, as with so many other quality-of-life improvements, comes not from heroic measures, but by assuring adequate access. And the market is a terrible mechanism for assuring such adequacy.
The reason we don’t have universal healthcare is mostly racism and male supremacy. Racist white people dont want anyone with dark skin getting a “free ride”. And, supporters of patriarchy don’t want their stay-at-home wives to be able to get healthcare without going through them because it undermines the husband’s power and control. They will use the language of “personal responsibility” or “free markets” to describe it, but the same people who don’t want universal healthcare also wave confederate flags and think that a woman’s place is in the home.
I was expecting to get downvoted for this, but it’s still true. In countries where women can get free childcare and free healthcare, they have more power. American men deeply fear this. In the end, like everything else, it’s all about power- who has it, who doesn’t. Big healthcare also makes a killing on the situation, but here in the states conservatives have always been willing to make the devils bargain of allying themselves with the ruling class in order to preserve white supremacy and male supremacy. It’s true no matter how many downvotes I get.
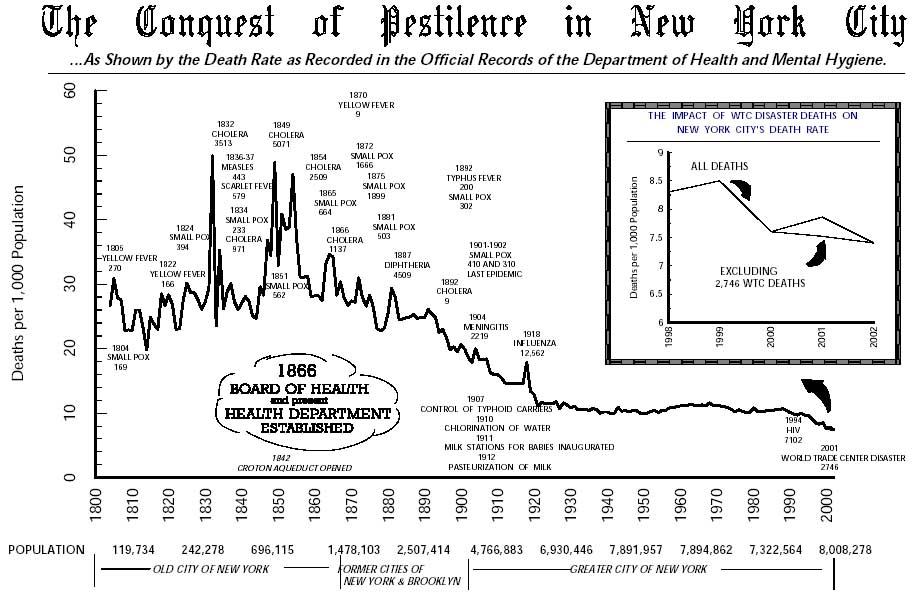{kind=link}
I have yet to hear a coherent explanation for how anyone can reasonably expect for price discovery to even pretend to function in a market where the consumers can't even guess the prices until after they've already purchased and frequently couldn't reasonably be expected to refuse service even if they did believe it was overpriced.